
Tue, May 7, 2024
[Archive]
Volume 7, Issue 4 (NOV 2022)
JNFS 2022, 7(4): 562-574 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Yaghoubi F, Darabi Z, Ahmadi Vasmehjani A, Sangsefidi Z S, Hosseinzadeh M. The Effect of Dark Chocolate on C-Reactive Protein Level: A Systematic Review and Meta-Analysis of Randomized Controlled Clinical Trials. JNFS 2022; 7 (4) :562-574
URL: http://jnfs.ssu.ac.ir/article-1-531-en.html
URL: http://jnfs.ssu.ac.ir/article-1-531-en.html
Fatemeh Yaghoubi 

 , Zahra Darabi , Azam Ahmadi Vasmehjani , Zohreh Sadat Sangsefidi , Mahdieh Hosseinzadeh *
, Zahra Darabi , Azam Ahmadi Vasmehjani , Zohreh Sadat Sangsefidi , Mahdieh Hosseinzadeh *
, Zahra Darabi , Azam Ahmadi Vasmehjani , Zohreh Sadat Sangsefidi , Mahdieh Hosseinzadeh *
Department of Nutrition, School of Public Health, Shahid Sadoughi University of Medical Sciences, Yazd, Iran
Full-Text [PDF 788 kb]
(228 Downloads)
| Abstract (HTML) (1260 Views)
Introduction
Full-Text: (196 Views)
The Effect of Dark Chocolate on C-Reactive Protein Level: A Systematic Review and Meta-Analysis of Randomized Controlled Clinical Trials
Fatemeh Yaghoubi; PhD 1,2, Zahra Darabi; PhD 2,3, Azam Ahmadi Vasmehjani; PhD 2,3,
Zohreh Sadat Sangsefidi; PhD 2,3,4 & Mahdieh Hosseinzadeh; PhD 2,3
Fatemeh Yaghoubi; PhD 1,2, Zahra Darabi; PhD 2,3, Azam Ahmadi Vasmehjani; PhD 2,3,
Zohreh Sadat Sangsefidi; PhD 2,3,4 & Mahdieh Hosseinzadeh; PhD 2,3
1 Department of Clinical Biochemistry, School of Medicine, Shahid Sadoughi University of Medical Sciences, Yazd,
Iran; 2 Nutrition and Food Security Research Center, School of Public Health, Shahid Sadoughi University of Medical Sciences, Yazd, Iran; 3 Department of Nutrition, School of Public Health, Shahid Sadoughi University of Medical Sciences, Yazd, Iran; 4 Department of Nutrition, School of Public Health, North Khorasan University of Medical Sciences, Bojnurd, Iran.
Iran; 2 Nutrition and Food Security Research Center, School of Public Health, Shahid Sadoughi University of Medical Sciences, Yazd, Iran; 3 Department of Nutrition, School of Public Health, Shahid Sadoughi University of Medical Sciences, Yazd, Iran; 4 Department of Nutrition, School of Public Health, North Khorasan University of Medical Sciences, Bojnurd, Iran.
.
| ARTICLE INFO | ABSTRACT | |
| SYSTEMATIC REVIEW and META-ANALYSIS | Background: This systematic review and meta‐analysis of randomized controlled trials (RCTs) was conducted to determine the effect of dark chocolate on C-Reactive Protein (CRP) levels as one of the inflammatory factors. Methods: A literature search was conducted in PubMed, ISI Web of Science, Scopus, and Google Scholar up to April of 2020. The registration number of study in PROSPERO was CRD4202020072, which was conducted over 5 eligible RCTs containing a total of 330 participants. The weighted mean difference (WMD) with 95% confidence intervals was calculated for the pool effect size of CRP. The heterogeneity of studies was examined by Cochran's Q test and I-squared (I2) statistic. Results: Effect sizes from 330 participants based on random effect model showed no effect between consumption of dark chocolate on CRP levels compared to the control group (WMD: 0.01 mg/dl; 95% CI: −0.19, 0.22 mg/dl; P = 0.89; Cochran's Q test, Q statistic = 21.97; P < 0.001; I2 = 81.80%). The results of subgroup analysis based on intervention duration and dosage showed no significant effect on CRP levels (WMD = 0.05 mg/dl, 95% CI: −0.30, 0.42 mg/dl; P = 0.76). Meta-regression for the intervention duration (slope: −0.0033, 95% CI: −0.0089, 0.0022; P = 0.24) and dosage (slope: 0.00006, 95% CI: −0.0036, 0.0037; P = 0.97) indicated no significant relationship with the mean difference of CRP. Conclusion: The results of the present meta-analysis showed that consuming dark chocolate had no significant effect on the CRP level. More clinical trials are required with higher quality and bigger sample sizes to verify the positive impact of dark chocolate on the reduction CRP level. Keywords: Dark chocolate; CRP; Inflammation |
|
| Article history: Received:2 Dec 2021 Revised: 4 Apr 2021 Accepted: 24 Apr 2021 |
||
| *Corresponding author: hoseinzade.mahdie@gmail.com Department of Nutrition, School of Public Health, Shahid Sadoughi University of Medical Sciences, Yazd, Iran. Postal code: 8915173160 Tel: + 98 35-31492232 |
Introduction
Inflammation increased the risk of cardiovascular diseases, certain cancer, metabolic diseases, such as obesity, metabolic syndrome, and type 2 diabetes (Hotamisligil et al., 1993, Mizuno et al., 2011, Nahrendorf and Swirski, 2015, Wellen and Hotamisligil, 2005). Previous studies have shown that inflammation can develop atherosclerosis, insulin resistance, endoplasmic reticular stress, and alternative gut microbiota. It also plays a role in the pathology of diseases, such as diabetes, cardiovascular disease, and obesity (Fernández-Real and Ricart, 2003, Hotamisligil, 2010, Tlaskalová-Hogenová et al., 2011). Oxidative stress is associated with inflammation in the body, leading to activation of nuclear factor-kB (NF-kB) and increasing transcription genes related to inflammatory cytokines production (Javadi et al., 2017). C-reactive protein (CRP) is a recognized marker of systemic inflammation that decreases the production of nitric oxide by endothelial cells and also affects the renin-angiotensin system. Reports have shown that CRP could affect progressive endothelial inflammation and atherosclerosis (Cottone et al., 2006).
Dark chocolate (DC) is one of the cocoa products, including cocoa butter and bean solids (up to 80% of the total weight) (Montagna et al., 2019). Results of meta-analysis have shown that consuming chocolate or cocoa improved endothelial function and reduced insulin resistance and blood pressure in adults (Hooper et al., 2012). Cocoa and dark chocolate contain flavonoids that have antioxidant and anti-inflammatory properties (Magrone et al., 2017). Several in vitro studies have reported that cocoa polyphenols could reduce the transcription and secretion of pro-inflammatory cytokines in human peripheral blood mononuclear cells (PBMCs), macrophages, and lymphoid cell lines (Mao et al., 2003, Ramiro et al., 2005). Results of some studies have shown that consumption of DC improves oxidative stress marker and has the potential to reduce oxidative stress (Malhi and Loomba, 2016, Nanetti et al., 2012).
Several clinical trials have reported the protective effects of DC on blood pressure (Desch et al., 2010, Haber and Gallus, 2012, Sudarma et al., 2011), glycemic factors (Grassi et al., 2008), and lipid profiles (Nanetti et al., 2008, Rezazadeh et al., 2015), while there are some controversial findings regarding the effect of DC on CRP. A study assessed the effect of DC on CRP level in 28 healthy volunteers. Results of this study showed that DC reduced high sensitivity-CRP levels (Hamed et al., 2008). However, some studies have represented no significant changes in CRP level after consuming DC (Di Renzo et al., 2013, Rezazadeh et al., 2015). To the best of the authors’ knowledge, no systematic review and meta‐analysis of randomized controlled trials (RCTs) have examined the effect of DC supplementation on CRP. Therefore, this meta‐analysis was conducted to summarize the up‐to‐date current evidence of RCTs, estimating the effect of DC supplementation on CRP as a biomarker of inflammation.
Materials and Methods
Search strategy: The present systematic review and meta-analysis was accomplished according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Guidelines (PRISMA) (Moher et al., 2015). The protocol of this study was registered in PROSPERO, an International Prospective Register of Systematic Reviews (http://www.crd.york.ac.uk/ PROSPERO) with the registration number of CRD42020200722. PubMed, ISI Web of Science, Scopus, and Google Scholar were searched up to 4 February 2022 without any restrictions to find eligible studies. Medical Subject Heading (MeSH) terms and non-MeSH terms were applied to investigate the effect of DC supplementation on CRP. The following keywords were used to search: ((chocolate[mesh] OR chocolate[tiab] OR “dark chocolate”[tiab]) AND (“c-reactive protein”[mesh] OR “c-reactive protein”[tiab] OR CRP[tiab] OR “hs-CRP”[tiab] OR inflammation[mesh] OR inflammation[tiab] OR “inflammatory markers”[tiab] OR “inflammatory biomarkers”[tiab] OR “inflammatory factors”[tiab] OR “inflammatory mediators”[tiab] OR “inflammatory indices”[tiab]))
To widen the search scope, the trial registries of the Iranian Registry of Clinical Trials and ClinicalTrials.gov were checked to identify unpublished trials in this context. In addition, the references list of the included trials was checked for further possible sources to ensure the comprehensiveness of searches.
Selection criteria: The selected studies had the following criteria: (1) had RCT design, (2) evaluated the impact of DC supplementation on CRP versus placebo/control, (3) presented the prescribed dosage, (4) included participants aged ≥18 years, and (5) provided sufficient information on CRP levels (serum or plasma) at the beginning and end of study (or its changes).
Study selection: The initial screening was carried out via two independent researchers (Yaghoubi F and Darabi Z), who studied the articles titles and abstracts. Then, the full texts of all related articles were evaluated via reviewers to select the trials about the effect of supplementation on CRP levels. Eventually, any possible disagreement was solved by consulting with the other researchers (Ahmadi Vasmehjani A and Sangsefidi ZS) (Figure 1).
Data extraction: Data extraction was conducted from the selected studies based on the following items: authors' family names; publication year; sample size; loss to follow-up; a dose of intervention; study duration; crossover or parallel study design; participants' gender, age, and health status; mean and standard deviation (SD) of CRP level at the beginning and at the end of the study, as well as the mean changes and SD of CRP level.
Risk of bias assessment: Evaluating the risk of bias of the included trials was conducted according to the Cochrane criteria (Higgins et al., 2019). The following items were applied for assessing the risk of bias of each research: (1) random sequence generation; (2) allocation concealment; (3) blinding of participants and personnel; (4) blinding of outcome assessment; (5) incomplete outcome data; (6) selective outcome reporting; and (7) other potential sources of bias. Based on the Cochrane Handbook recommendations, studies were rated on each item as “yes” demonstrating the low risk of bias, “no” indicating a high risk of bias, or “unclear” when the risk of bias was unclear or unknown. Additionally, by identifying the six domains as the most important ones (‘key domains’), each trial was specified an overall risk of bias in terms of low risk (low for all key domains), high risk (high for one or more key domains.), and unclear risk (unclear for one or more key domains).
Ethics approval and consent to participate: This is a systematic review and meta-analysis which was conducted based on prior studies, so ethical approval is not mentioned. The protocol of this study was registered in PROSPERO, an International Prospective Register of Systematic Reviews (http://www.crd.york.ac.uk/PROSPERO) with the registration number of CRD42020200722.
Data synthesis and analysis: The difference in means was determined as effect sizes. The weighted mean differences (WMDs) were computed as follows: mean divided by the standard deviation of a difference between two random values each from one of two groups (Higgins, 2011). In studies that the standard error (SE) value had been presented, SD was obtained by the following formula: SD = SE×√n (n=number of participants in each group). The random-effects model was used to calculate the WMDs with 95% confidence intervals (CIs) for conducting the meta-analysis, which took the between-study heterogeneity into account (Borenstein et al., 2011). Moreover, heterogeneity of studies was examined by Cochran's Q test and I-squared (I2) statistic. Heterogeneity was specified as follow: Q statistic P-value of < 0.1; weak heterogeneity: I2 = 25-50, relatively high heterogeneity: I2 = 50-75, high heterogeneity: I2 = 75-100 (Higgins and Thompson, 2002). To identify the possible sources of heterogeneity in the included studies, Subgroup analysis was performed. Given that the administered intervention dosage and duration trial might affect the findings regarding the effect of DC, sub-group analysis was accomplished based on these variables. Publication bias was also examined by assessing the funnel plot and asymmetry tests, including Begg’s rank correlation test and Egger’s regression test (using P-value of < 0.05) (Duval and Tweedie, 2000). Furthermore, a sensitivity analysis was performed to determine the effect of a specific study or a particular group of studies via individual removal of each study or a specific group and recalculation of the pooled estimates. Meta-regression was also performed to evaluate the association of the estimated effect size with dark chocolate dosage and study duration. Statistical analyses were accomplished by CMA software, version 11.2 (STATA Corp.). Statistically significant levels were specified as P < 0.05.
Results
Study selection: In the initial search, according to the search designs from electronic medical databases, 647 articles were found (Figure 1). The search strategy is shown in the supplementary material. After removing duplicates, 421 studies remained. From this number, 416 articles were excluded because they were not clinical trials (n = 376) or did not meet the inclusion criteria (n = 37) and or not found in medical databases (n = 3). Finally, 5 eligible studies included in this meta-analysis.
Characteristics of the studies: The details of the 5 included studies are presented in Table 1. Studies were listed based on the following information: country, age (y), gender, sample size (intervention), RCT design, intervention name, the dosage of DC, name control, duration, outcome, the health status of participants. Studies were published from 2005 to 2018 and the sample size ranged from 19 to 110 participants. A cross-over design was in three studies (da Costa Teixeira et al., 2017, Grassi et al., 2008, Grassi et al., 2005), one study had parallel -4 armed design (Kurlandsky and Stote, 2006) and so one was a randomized clinical trial (Jafarirad et al., 2018). The intervention duration in the trials was 15-56 days. The dose of DC in the intervention groups was from 30 to 100 g/day. All studies except one trial reported mean ± SD for CRP levels at the start and end of the trial in two groups of intervention and placebo. Two studies were conducted in Italy (Grassi et al., 2008, Grassi et al., 2005) and one in every one of the following countries, Brazile (da Costa Teixeira et al., 2017), USA (Kurlandsky and Stote, 2006), Iran (Jafarirad et al., 2018).
Quality assessment of the studies: The quality assessment of the included articles is summarized in Table 2. Briefly, all studies were categorized as low risk of bias for incomplete outcome data and selective reporting. Random sequence generation was described only in one study (Jafarirad et al., 2018), but a lack of information was observed in other studies. Three studies were considered low risk of bias for allocation concealment (Grassi et al., 2008, Jafarirad et al., 2018, Kurlandsky and Stote, 2006) and the remaining two studies did not express any method for allocation concealment; therefore, they were regarded as unclear risk of bias (da Costa Teixeira et al., 2017, Grassi et al., 2005). Two studies did not report the use of any method for blinding of participants and personnel and selective reporting (Grassi et al., 2005, Kurlandsky and Stote, 2006). The blinding of outcome assessment was unclear in all studies. Three included studies were at least 1 of the 6 key domains of unclear risk of bias, thus overall quality was unclear (da Costa Teixeira et al., 2017, Grassi et al., 2008, Jafarirad et al., 2018). Two studies had at least 1 of the 6 key domains of high risk of bias; therefore, their overall quality became the high risk of bias (Grassi et al., 2005, Kurlandsky and Stote, 2006).
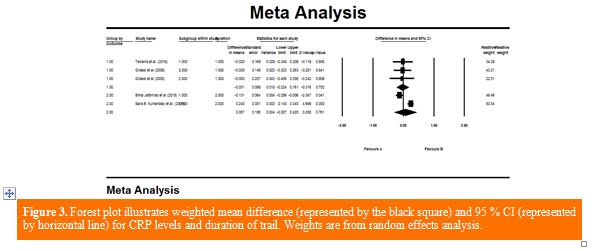
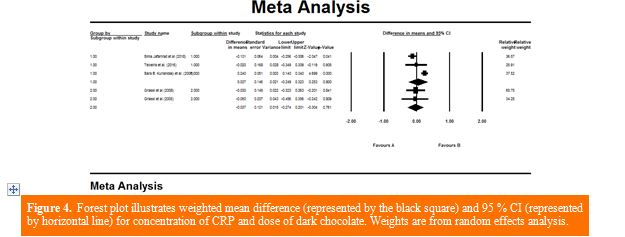
Finding from meta-analysis: Combining 5 effect sizes from 5 studies (n = 376) based on random effect model showed no effect of consuming DC on CRP levels compared to the control group WMD: 0.014 mg/dl; 95% CI: −0.19, 0.22 mg/dl; P = 0.89; Cochran's Q test, Q statistic = 21.97; P <0.001; I2 = 81.80%] (Figure 2). Sensitivity analysis was accomplished to evaluate the effect of each study individually on the overall findings; each trial was removed but did not change meta-analysis results. The findings of subgroup analysis based on intervention duration and dosage disclosed no significant effect on CRP levels (WMD = 0.05 mg/dl, 95% CI: −0.30, 0.42 mg/dl; P = 0.76) and (WMD = −0.03 mg/dl, 95% CI: −0.27, 0.20 mg/dl; P = 0.76), respectively (Figures 3 and 4).
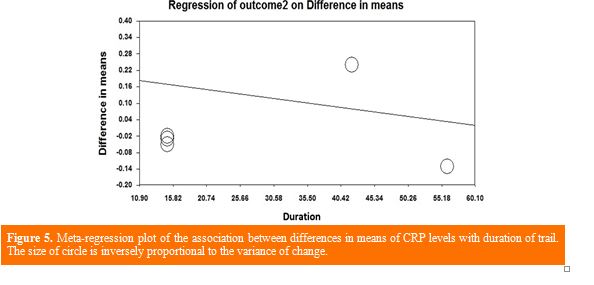
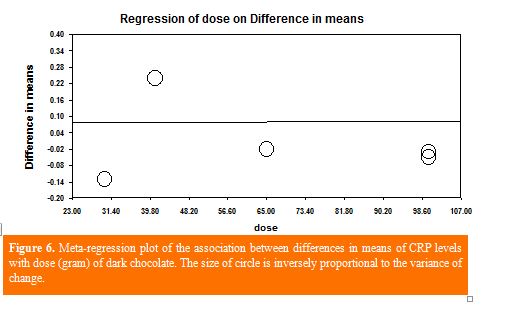
Meta‐regression analysis based on all studies was implemented to investigate the linear association between DC duration and dosage with the mean difference of CRP levels. Meta-regression for the intervention duration (slope: −0.0033, 95% CI: −0.0089, 0.0022; P = 0.24) and dosage (slope: 0.00006, 95% CI: −0.0036, 0.0037; P = 0.97) did not indicate any significant relevance with the mean difference of CRP (Figures 5 and 6).
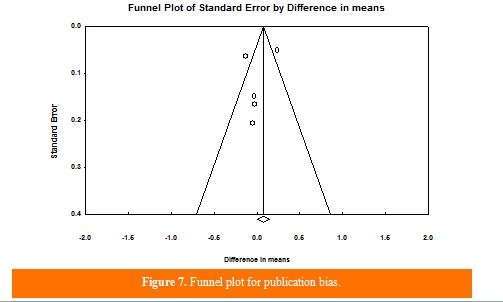
Although the asymmetric statistical tests did not show the existence of a publishing bias for the meta‐analysis of CRP (Begg's test, P = 1; Egger's regression test, P = 0.51), the funnel plot indicated a visual publication bias )Figure7). After adjusting the effect size for publication bias by the" trim and fill" correction, no potentially missing surveys were needed in the funnel plot (WMD= 0.01 mg/dl, 95%CI= -0.19-0.22 mg/dl).
.JPG)

Dark chocolate (DC) is one of the cocoa products, including cocoa butter and bean solids (up to 80% of the total weight) (Montagna et al., 2019). Results of meta-analysis have shown that consuming chocolate or cocoa improved endothelial function and reduced insulin resistance and blood pressure in adults (Hooper et al., 2012). Cocoa and dark chocolate contain flavonoids that have antioxidant and anti-inflammatory properties (Magrone et al., 2017). Several in vitro studies have reported that cocoa polyphenols could reduce the transcription and secretion of pro-inflammatory cytokines in human peripheral blood mononuclear cells (PBMCs), macrophages, and lymphoid cell lines (Mao et al., 2003, Ramiro et al., 2005). Results of some studies have shown that consumption of DC improves oxidative stress marker and has the potential to reduce oxidative stress (Malhi and Loomba, 2016, Nanetti et al., 2012).
Several clinical trials have reported the protective effects of DC on blood pressure (Desch et al., 2010, Haber and Gallus, 2012, Sudarma et al., 2011), glycemic factors (Grassi et al., 2008), and lipid profiles (Nanetti et al., 2008, Rezazadeh et al., 2015), while there are some controversial findings regarding the effect of DC on CRP. A study assessed the effect of DC on CRP level in 28 healthy volunteers. Results of this study showed that DC reduced high sensitivity-CRP levels (Hamed et al., 2008). However, some studies have represented no significant changes in CRP level after consuming DC (Di Renzo et al., 2013, Rezazadeh et al., 2015). To the best of the authors’ knowledge, no systematic review and meta‐analysis of randomized controlled trials (RCTs) have examined the effect of DC supplementation on CRP. Therefore, this meta‐analysis was conducted to summarize the up‐to‐date current evidence of RCTs, estimating the effect of DC supplementation on CRP as a biomarker of inflammation.
Materials and Methods
Search strategy: The present systematic review and meta-analysis was accomplished according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Guidelines (PRISMA) (Moher et al., 2015). The protocol of this study was registered in PROSPERO, an International Prospective Register of Systematic Reviews (http://www.crd.york.ac.uk/ PROSPERO) with the registration number of CRD42020200722. PubMed, ISI Web of Science, Scopus, and Google Scholar were searched up to 4 February 2022 without any restrictions to find eligible studies. Medical Subject Heading (MeSH) terms and non-MeSH terms were applied to investigate the effect of DC supplementation on CRP. The following keywords were used to search: ((chocolate[mesh] OR chocolate[tiab] OR “dark chocolate”[tiab]) AND (“c-reactive protein”[mesh] OR “c-reactive protein”[tiab] OR CRP[tiab] OR “hs-CRP”[tiab] OR inflammation[mesh] OR inflammation[tiab] OR “inflammatory markers”[tiab] OR “inflammatory biomarkers”[tiab] OR “inflammatory factors”[tiab] OR “inflammatory mediators”[tiab] OR “inflammatory indices”[tiab]))
To widen the search scope, the trial registries of the Iranian Registry of Clinical Trials and ClinicalTrials.gov were checked to identify unpublished trials in this context. In addition, the references list of the included trials was checked for further possible sources to ensure the comprehensiveness of searches.
Selection criteria: The selected studies had the following criteria: (1) had RCT design, (2) evaluated the impact of DC supplementation on CRP versus placebo/control, (3) presented the prescribed dosage, (4) included participants aged ≥18 years, and (5) provided sufficient information on CRP levels (serum or plasma) at the beginning and end of study (or its changes).
Study selection: The initial screening was carried out via two independent researchers (Yaghoubi F and Darabi Z), who studied the articles titles and abstracts. Then, the full texts of all related articles were evaluated via reviewers to select the trials about the effect of supplementation on CRP levels. Eventually, any possible disagreement was solved by consulting with the other researchers (Ahmadi Vasmehjani A and Sangsefidi ZS) (Figure 1).
Data extraction: Data extraction was conducted from the selected studies based on the following items: authors' family names; publication year; sample size; loss to follow-up; a dose of intervention; study duration; crossover or parallel study design; participants' gender, age, and health status; mean and standard deviation (SD) of CRP level at the beginning and at the end of the study, as well as the mean changes and SD of CRP level.
Risk of bias assessment: Evaluating the risk of bias of the included trials was conducted according to the Cochrane criteria (Higgins et al., 2019). The following items were applied for assessing the risk of bias of each research: (1) random sequence generation; (2) allocation concealment; (3) blinding of participants and personnel; (4) blinding of outcome assessment; (5) incomplete outcome data; (6) selective outcome reporting; and (7) other potential sources of bias. Based on the Cochrane Handbook recommendations, studies were rated on each item as “yes” demonstrating the low risk of bias, “no” indicating a high risk of bias, or “unclear” when the risk of bias was unclear or unknown. Additionally, by identifying the six domains as the most important ones (‘key domains’), each trial was specified an overall risk of bias in terms of low risk (low for all key domains), high risk (high for one or more key domains.), and unclear risk (unclear for one or more key domains).
Ethics approval and consent to participate: This is a systematic review and meta-analysis which was conducted based on prior studies, so ethical approval is not mentioned. The protocol of this study was registered in PROSPERO, an International Prospective Register of Systematic Reviews (http://www.crd.york.ac.uk/PROSPERO) with the registration number of CRD42020200722.
Data synthesis and analysis: The difference in means was determined as effect sizes. The weighted mean differences (WMDs) were computed as follows: mean divided by the standard deviation of a difference between two random values each from one of two groups (Higgins, 2011). In studies that the standard error (SE) value had been presented, SD was obtained by the following formula: SD = SE×√n (n=number of participants in each group). The random-effects model was used to calculate the WMDs with 95% confidence intervals (CIs) for conducting the meta-analysis, which took the between-study heterogeneity into account (Borenstein et al., 2011). Moreover, heterogeneity of studies was examined by Cochran's Q test and I-squared (I2) statistic. Heterogeneity was specified as follow: Q statistic P-value of < 0.1; weak heterogeneity: I2 = 25-50, relatively high heterogeneity: I2 = 50-75, high heterogeneity: I2 = 75-100 (Higgins and Thompson, 2002). To identify the possible sources of heterogeneity in the included studies, Subgroup analysis was performed. Given that the administered intervention dosage and duration trial might affect the findings regarding the effect of DC, sub-group analysis was accomplished based on these variables. Publication bias was also examined by assessing the funnel plot and asymmetry tests, including Begg’s rank correlation test and Egger’s regression test (using P-value of < 0.05) (Duval and Tweedie, 2000). Furthermore, a sensitivity analysis was performed to determine the effect of a specific study or a particular group of studies via individual removal of each study or a specific group and recalculation of the pooled estimates. Meta-regression was also performed to evaluate the association of the estimated effect size with dark chocolate dosage and study duration. Statistical analyses were accomplished by CMA software, version 11.2 (STATA Corp.). Statistically significant levels were specified as P < 0.05.
Results
Study selection: In the initial search, according to the search designs from electronic medical databases, 647 articles were found (Figure 1). The search strategy is shown in the supplementary material. After removing duplicates, 421 studies remained. From this number, 416 articles were excluded because they were not clinical trials (n = 376) or did not meet the inclusion criteria (n = 37) and or not found in medical databases (n = 3). Finally, 5 eligible studies included in this meta-analysis.
Characteristics of the studies: The details of the 5 included studies are presented in Table 1. Studies were listed based on the following information: country, age (y), gender, sample size (intervention), RCT design, intervention name, the dosage of DC, name control, duration, outcome, the health status of participants. Studies were published from 2005 to 2018 and the sample size ranged from 19 to 110 participants. A cross-over design was in three studies (da Costa Teixeira et al., 2017, Grassi et al., 2008, Grassi et al., 2005), one study had parallel -4 armed design (Kurlandsky and Stote, 2006) and so one was a randomized clinical trial (Jafarirad et al., 2018). The intervention duration in the trials was 15-56 days. The dose of DC in the intervention groups was from 30 to 100 g/day. All studies except one trial reported mean ± SD for CRP levels at the start and end of the trial in two groups of intervention and placebo. Two studies were conducted in Italy (Grassi et al., 2008, Grassi et al., 2005) and one in every one of the following countries, Brazile (da Costa Teixeira et al., 2017), USA (Kurlandsky and Stote, 2006), Iran (Jafarirad et al., 2018).
Quality assessment of the studies: The quality assessment of the included articles is summarized in Table 2. Briefly, all studies were categorized as low risk of bias for incomplete outcome data and selective reporting. Random sequence generation was described only in one study (Jafarirad et al., 2018), but a lack of information was observed in other studies. Three studies were considered low risk of bias for allocation concealment (Grassi et al., 2008, Jafarirad et al., 2018, Kurlandsky and Stote, 2006) and the remaining two studies did not express any method for allocation concealment; therefore, they were regarded as unclear risk of bias (da Costa Teixeira et al., 2017, Grassi et al., 2005). Two studies did not report the use of any method for blinding of participants and personnel and selective reporting (Grassi et al., 2005, Kurlandsky and Stote, 2006). The blinding of outcome assessment was unclear in all studies. Three included studies were at least 1 of the 6 key domains of unclear risk of bias, thus overall quality was unclear (da Costa Teixeira et al., 2017, Grassi et al., 2008, Jafarirad et al., 2018). Two studies had at least 1 of the 6 key domains of high risk of bias; therefore, their overall quality became the high risk of bias (Grassi et al., 2005, Kurlandsky and Stote, 2006).
Finding from meta-analysis: Combining 5 effect sizes from 5 studies (n = 376) based on random effect model showed no effect of consuming DC on CRP levels compared to the control group WMD: 0.014 mg/dl; 95% CI: −0.19, 0.22 mg/dl; P = 0.89; Cochran's Q test, Q statistic = 21.97; P <0.001; I2 = 81.80%] (Figure 2). Sensitivity analysis was accomplished to evaluate the effect of each study individually on the overall findings; each trial was removed but did not change meta-analysis results. The findings of subgroup analysis based on intervention duration and dosage disclosed no significant effect on CRP levels (WMD = 0.05 mg/dl, 95% CI: −0.30, 0.42 mg/dl; P = 0.76) and (WMD = −0.03 mg/dl, 95% CI: −0.27, 0.20 mg/dl; P = 0.76), respectively (Figures 3 and 4).
Meta‐regression analysis based on all studies was implemented to investigate the linear association between DC duration and dosage with the mean difference of CRP levels. Meta-regression for the intervention duration (slope: −0.0033, 95% CI: −0.0089, 0.0022; P = 0.24) and dosage (slope: 0.00006, 95% CI: −0.0036, 0.0037; P = 0.97) did not indicate any significant relevance with the mean difference of CRP (Figures 5 and 6).
Although the asymmetric statistical tests did not show the existence of a publishing bias for the meta‐analysis of CRP (Begg's test, P = 1; Egger's regression test, P = 0.51), the funnel plot indicated a visual publication bias )Figure7). After adjusting the effect size for publication bias by the" trim and fill" correction, no potentially missing surveys were needed in the funnel plot (WMD= 0.01 mg/dl, 95%CI= -0.19-0.22 mg/dl).
Table 1. General characteristics of the included studies. |
||||||||||||
| Status of health | Duration ( day ) | Outcome | Con | Dosage of dark chocolate (g/day) |
Int name and dose | RCT Design |
Sample size(int) | Gender | Age (y) | Country | First Author (year) | |
| Con | Int | |||||||||||
| Never treated essential hypertensive |
15 |
CRP before: 0.35 ± 0.31 mg/dl; after: 0.36 ± 0.31 mg/dl | CRP before: 0.37 ± 0.39a mg/dl; after: 0.33 ± 0.39 mg/dl | Flavanol-free white chocolate |
100 |
Flavanol-rich dark chocolate |
Crossover |
35(20) |
F/M |
25-60 |
Italy |
Grassi et al. (2005) |
| Healthy |
42 |
b -1.3±1.2 |
1.1±1.3 b |
Self-selected diet avoiding nuts and chocolate | 41 |
Dark chocolate daily with a self-selected diet |
Parallel 4-armed |
24(12) |
F |
22-65 |
USA |
Sara B. Kurlandsky et al. (2006) |
| Hypertensive with IGT |
15 |
CRP before: 0.37 ± 0.23 mg/dl; after: 0.36 ± 0.14 mg/dl | CRP before: 0.38 ± 0.26 mg/dl; after: 0.34 ± 0.33 mg/dl | Flavanol-free white chocolate |
100 |
Flavanol-rich dark chocolate |
Crossover |
38(19) |
F/M |
mean: 44.8 |
Italy |
Grassi et al. (2008) |
| HIV/AIDS undergoing ART |
15 |
CRP before: 0.33 ± 0.81 mg/dl; after: 0.30 ± .57 mg/dl |
CRP before: 0.33 ± 0.81 mg/dl; after: 0.28 ± 0.34 mg/dl |
White chocolate |
65 |
Chocolate bar containing 36 g cocoa (2864 mg polyphenols | Crossover double-blind |
110(53) |
F/M |
Range: 19-59 |
Brazil |
Teixeira et al. (2016) |
| Diabetes |
56 |
CRP before: 0.32 ± 0.13 mg/dl; after: 0.42± 0.16 mg/dl | CRP before: 0.42 ± 0.12 mg/dl; after: 0.39 ± 0.21 mg/dl | Only TLC guidelines |
30 |
Dark chocolate |
RCT Parallel |
44(21) |
F/M |
30-60 |
Iran |
Sima Jafarirad et al. (2018) |
| F: female, M: male; RCT: randomized controlled trial; int: intervention; con: control; CRP: C-reactive protein; IGT: Impaired glucose tolerance; ART: Antiviral therapy; TLC: Therapeutic lifestyle change; a: mean ±SD; b: Changes in circulating levels of CRP |
||||||||||||
Table 2. Risk of bias assessment according to the Cochrane collaboration tool. |
|||||||
| First author (year) | Random sequence generation |
Allocation concealment |
Blinding of participants and personnel |
Blinding of outcome assessment |
Incomplete outcome data |
Selective reporting |
Summary of overall assessment |
| Grassi et al. (2005) | U | U | H | U | L | L | H |
| Sara B.Kurlandsky et al. (2006) | U | L | H | U | L | L | H |
| Grassi et al. (2008) | U | L | L | U | L | L | U |
| Teixeira et al. (2016) | U | U | L | U | L | L | U |
| Sima Jafarirad et al. (2018) | L | L | L | U | L | L | U |
| H: high risk; L: low risk; U: unclear | |||||||
Discussion
The study findings indicate that DC supplementation has any significant effects on the level of CRP. This result was independent of doses and duration of chocolate intake. Altogether among 5 surveys, the results of 4 studies (da Costa Teixeira et al., 2017, Grassi et al., 2008, Grassi et al., 2005, Jafarirad et al., 2018) showed a negative relationship between DC and the level of CRP. In contrast, the study by Sara B. Kurlandsky et al. is inconsistent with the total result of the present study (Kurlandsky and Stote, 2006). However, sensitivity analysis did not represent any sensitivity to these studies.
To the best of the authors’ knowledge, the present systematic review and meta-analysis is the first study on the effects of dark chocolate on CRP. Inconsistent with the present study results, a recent meta-analysis assessed the effect of cocoa/dark chocolate supplementation on body weight, body mass index, and waist circumference, which reported no significant effect (Kord-Varkaneh et al., 2019). Another meta-analysis examined the effect of cocoa products as a source of DC on serum lipids. Intervention with cocoa products significantly reduced serum low-density lipoprotein (LDL) and total cholesterol (TC) levels, while it did not have any significant effects on high-density lipoprotein (HDL) similar to the current study, although no significant change was observed in LDL cholesterol in high-quality studies (3 studies) (Jia et al., 2010). Mehrabani et al. conducted a meta-analysis on the impact of cocoa consumption on markers of oxidative stress. They reported that malondialdehyde and 8-iso-prostaglandin F2α were significantly reduced, but not in other markers of oxidative stress (Mehrabani et al., 2020).
Consequently, several factors can lead to these controversial results, including different dosages and duration of DC, sample sizes of studies, the diverse status of subjects' health, and initial levels of CRP (Haghighat et al., 2013, Sangsefidi et al., 2020). Also depending on the concentration of dark chocolates' polyphenols and free radical sources, the role of polyphenols could differ between antioxidants and pro-oxidants and subsequently act as either anti-inflammatory or pro-inflammatory compounds (Cao et al., 1997, Di Giuseppe et al., 2008).
The role of inflammation in the pathogenesis of many chronic diseases, such as different cancers diabetes and cardiovascular disease is undeniable (Libby, 2007). On the other hand, many studies represent the protective role of flavonols on the inflammatory pathway (Kuebler et al., 2016, Selmi et al., 2008). The underlying mechanisms by which DC can attenuate inflammatory responses include inhibition of cyclooxygenase-2, prevention of the activation of T-cell and B-cells, reducing the expression and secretion of Interleukin 2, and reducing the amount and properties of inflammatory cytokines (IL5, TNF-α, TGF-β) (Haghighat et al., 2013, Mao et al., 2000, Sanbongi et al., 1997). Possibly DC can mediate these events via transcription factors, such as nuclear transcription factor-kB (NF-kB), affecting the transcription and secretion of many cytokines (Mao et al., 2000).
The advantages of the present study include using advanced search strategies, lack of linguistic restrictions in the search process, quality assessment based on Cochrane criteria, and different subgroup analyses according to duration and dosage of supplementation. However, there are some limitations, including the low quality of the related clinical trials and the significant heterogeneity, resulting from different doses of DC (22-100 g/day), supplemental period (15-56 days), different study size (20-158), and diverse characteristics of participants, such as health status, age, and gender. On the other hand, owing to the high publication bias, caution needs to be considered about the result of this study.
The current study results reveal that the treatment with DC had no significant effect on the CRP level. Due to the controversial finding of the conducted clinical trials, more studies with more quality and bigger sample sizes are required to verify the positive impact of DC in reducing CRP level.
Acknowledgment
Thanks are owed to the Nutrition and Food Security Research Center in Shahid Sadoughi University of Medical Sciences in Yazd, Iran, for supporting this study.
Conflict of interest
The authors declare no conflict of interest.
Funding
There was no role of the funding in the preparation of this study.
Authors’ contributions
Yaghoubi F and Darabi Z prepared the proposal, obtained ethical approvals, applied for
funding and Yaghoubi F, Ahmadi A, Darabi Z and Sangsefidi ZS wrote the manuscript and performed data analysis. Hosseinzadeh M conceived the idea and supervised the study. All authors read and approved the final manuscript.
References
Borenstein M, Hedges LV, Higgins JP & Rothstein HR 2011. Introduction to meta-analysis. John Wiley & Sons.
Cao G, Sofic E & Prior RL 1997. Antioxidant and prooxidant behavior of flavonoids: structure-activity relationships. Free radical biology and medicine. 22 (5): 749-760.
Cottone S, et al. 2006. Relation of C-reactive protein to oxidative stress and to endothelial activation in essential hypertension. American journal of hypertension. 19 (3): 313-318.
da Costa Teixeira AMN, et al. 2017. The impact of dark chocolate intake on arterial elasticity in individuals with HIV/AIDS undergoing ART: a randomized, double-blind, crossover trial. Food & function. 8 (6): 2212-2219.
Desch S, et al. 2010. Low vs. higher-dose dark chocolate and blood pressure in cardiovascular high-risk patients. American journal of hypertension. 23 (6): 694-700.
Di Giuseppe R, et al. 2008. Regular consumption of dark chocolate is associated with low serum concentrations of C-reactive protein in a healthy Italian population. Journal of nutrition. 138 (10): 1939-1945.
Di Renzo L, et al. 2013. Effects of dark chocolate in a population of normal weight obese women:a pilot study. European review for medical and pharmacological sciences. 17 (16): 2257-2266.
Duval S & Tweedie R 2000. Trim and fill: a simple funnel‐plot–based method of testing and adjusting for publication bias in meta‐analysis. Biometrics. 56 (2): 455-463.
Fernández-Real JM & Ricart W 2003. Insulin resistance and chronic cardiovascular inflammatory syndrome. Endocrine reviews. 24 (3): 278-301.
Grassi D, et al. 2008. Blood pressure is reduced and insulin sensitivity increased in glucose-intolerant, hypertensive subjects after 15 days of consuming high-polyphenol dark chocolate. Journal of nutrition. 138 (9): 1671-1676.
Grassi D, et al. 2005. Cocoa reduces blood pressure and insulin resistance and improves endothelium-dependent vasodilation in hypertensives. Hypertension. 46 (2): 398-405.
Haber SL & Gallus K 2012. Effects of dark chocolate on blood pressure in patients with hypertension. American journal of health-system pharmacy. 69 (15): 1287-1288, 1290, 1292-1283.
Haghighat N, et al. 2013. The effects of dark chocolate on lipid profile, apo-lipoprotein A-1, apo-lipoprotein B and inflammation in type-2 diabetic patients: A randomized clinical trial. Iranian journal of nutrition sciences & food technology. 8 (2): 21-30.
Hamed MS, et al. 2008. Dark chocolate effect on platelet activity, C-reactive protein and lipid profile: a pilot study. Southern medical journal. 101 (12): 1203-1208.
Higgins J 2011. GSE Cochrane Handbook for Systematic Systematic Reviews of Interventions Version 5.1. 0.
Higgins J, et al. 2019. Cochrane handbook for systematic reviews of interventions. John Wiley & Sons.
Higgins J & Thompson SG 2002. Quantifying heterogeneity in a meta‐analysis. Statistics in medicine. 21 (11): 1539-1558.
Hooper L, et al. 2012. Effects of chocolate, cocoa, and flavan-3-ols on cardiovascular health: a systematic review and meta-analysis of randomized trials. American journal of clinical nutrition. 95 (3): 740-751.
Hotamisligil GS 2010. Endoplasmic reticulum stress and the inflammatory basis of metabolic disease. Cell. 140 (6): 900-917.
Hotamisligil GS, Shargill NS & Spiegelman BM 1993. Adipose expression of tumor necrosis factor-alpha: direct role in obesity-linked insulin resistance. Science. 259 (5091): 87-91.
Jafarirad S, et al. 2018. Dark chocolate effect on serum adiponectin, biochemical and inflammatory parameters in diabetic patients: A randomized clinical trial. International journal of preventive medicine. 9.
Javadi F, et al. 2017. The effect of quercetin on inflammatory factors and clinical symptoms in women with rheumatoid arthritis: a double-blind, randomized controlled trial. Journal of the American college of nutrition. 36 (1): 9-15.
Jia L, et al. 2010. Short-term effect of cocoa product consumption on lipid profile: a meta-analysis of randomized controlled trials. American journal of clinical of nutrition. 92: 218-225.
Kord-Varkaneh H, Ghaedi E, Nazary-Vanani A, Mohammadi H & Shab-Bidar S 2019. Does cocoa/dark chocolate supplementation have favorable effect on body weight, body mass index and waist circumference? A systematic review, meta-analysis and dose-response
of randomized clinical trials. Critical reviews in food science and nutrition. 59 (15): 2349-2362.
Kuebler U, et al. 2016. Dark chocolate attenuates intracellular pro-inflammatory reactivity to acute psychosocial stress in men: A randomized controlled trial. Brain, behavior, and immunity. 57: 200-208.
Kurlandsky SB & Stote KS 2006. Cardioprotective effects of chocolate and almond consumption in healthy women. Nutrition research. 26 (10): 509-516.
Libby P 2007. Inflammatory mechanisms: the molecular basis of inflammation and disease. Nutrition reviews. 65 (12 Pt 2): S140-146.
Magrone T, Russo MA & Jirillo E 2017. Cocoa and dark chocolate polyphenols: from biology to clinical applications. Frontiers in immunology. 8: 677.
Malhi H & Loomba R 2016. Editorial: dark chocolate may improve NAFLD and metabolic syndrome by reducing oxidative stress. Alimentary pharmacology & therapeutics. 44 (5): 533-534.
Mao T, et al. 2000. Effect of cocoa procyanidins on the secretion of interleukin-4 in peripheral blood mononuclear cells. Journal of medicinal food. 3 (2): 107-114.
Mao T, Water JVD, Keen C, Schmitz H & Gershwin M 2003. Cocoa Flavonols and Procyanidins Promote Transforming Growth Factor-β1 Homeostasis in Peripheral Blood Mononuclear Cells1. Experimental biology and medicine. 228 (1): 93-99.
Mehrabani S, Arab A, Mohammadi H & Amani R 2020. The effect of cocoa consumption on markers of oxidative stress: A systematic review and meta-analysis of interventional studies. Complementary therapies in medicine. 48: 102240.
Mizuno Y, Jacob RF & Mason RP 2011. Inflammation and the development of atherosclerosis: effects of lipid-lowering therapy. Journal of atherosclerosis and thrombosis. 1103160359-1103160359.
Moher D, et al. 2015. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Systematic review. 4 (1): 1.
Montagna MT, et al. 2019. Chocolate,“food of the gods”: History, science, and human health. International journal of environmental research and public health. 16 (24): 4960.
Nahrendorf M & Swirski FK 2015. Neutrophil-macrophage communication in inflammation and atherosclerosis. Science. 349 (6245): 237-238.
Nanetti L, et al. 2012. Effect of consumption of dark chocolate on oxidative stress in lipoproteins and platelets in women and in men. Appetite. 58 (1): 400-405.
Nanetti L, et al. 2008. Effect of consumption of dark chocolate on lipoproteins and serum lipids. Mediterranean journal of nutrition and metabolism. 1 (1): 25.
Ramiro E, et al. 2005. Flavonoids from Theobroma cacao down-regulate inflammatory mediators. Journal of agricultural and food chemistry. 53 (22): 8506-8511.
Rezazadeh A, Mahmoodi M, Mard SA & karimi Moghaddam E 2015. The effects of dark chocolate consumption on lipid profile, fasting blood sugar, liver enzymes, inflammation, and antioxidant status in patients with non-alcoholic fatty liver disease: a randomized, placebo-controlled, pilot study. Journal of gastroenterology and hepatology research. 4 (12): 1858-1864.
Sanbongi C, Suzuki N & Sakane T 1997. Polyphenols in chocolate, which have antioxidant activity, modulate immune functions in humansin vitro. Cellular immunology. 177 (2): 129-136.
Sangsefidi ZS, Yaghoubi F, Hajiahmadi S & Hosseinzadeh M 2020. The effect of coenzyme Q10 supplementation on oxidative stress: A systematic review and meta‐analysis of randomized controlled clinical trials. Food science & nutrition. 8 (4): 1766-1776.
Selmi C, Cocchi CA, Lanfredini M, Keen CL & Gershwin ME 2008. Chocolate at heart: The anti‐inflammatory impact of cocoa flavanols. Molecular nutrition & food research. 52 (11): 1340-1348.
Sudarma V, Sukmaniah S & Siregar P 2011. Effect of dark chocolate on nitric oxide serum levels and blood pressure in prehypertension subjects. Acta medica Indonesiana. 43 (4): 224-228.
Tlaskalová-Hogenová H, et al. 2011. The role of gut microbiota (commensal bacteria) and the mucosal barrier in the pathogenesis of inflammatory and autoimmune diseases and cancer: contribution of germ-free and gnotobiotic animal models of human diseases. Cellular & molecular immunology. 8 (2): 110-120.
Wellen KE & Hotamisligil GS 2005. Inflammation, stress, and diabetes. Journal of clinical investigation. 115 (5): 1111-1119.
The study findings indicate that DC supplementation has any significant effects on the level of CRP. This result was independent of doses and duration of chocolate intake. Altogether among 5 surveys, the results of 4 studies (da Costa Teixeira et al., 2017, Grassi et al., 2008, Grassi et al., 2005, Jafarirad et al., 2018) showed a negative relationship between DC and the level of CRP. In contrast, the study by Sara B. Kurlandsky et al. is inconsistent with the total result of the present study (Kurlandsky and Stote, 2006). However, sensitivity analysis did not represent any sensitivity to these studies.
To the best of the authors’ knowledge, the present systematic review and meta-analysis is the first study on the effects of dark chocolate on CRP. Inconsistent with the present study results, a recent meta-analysis assessed the effect of cocoa/dark chocolate supplementation on body weight, body mass index, and waist circumference, which reported no significant effect (Kord-Varkaneh et al., 2019). Another meta-analysis examined the effect of cocoa products as a source of DC on serum lipids. Intervention with cocoa products significantly reduced serum low-density lipoprotein (LDL) and total cholesterol (TC) levels, while it did not have any significant effects on high-density lipoprotein (HDL) similar to the current study, although no significant change was observed in LDL cholesterol in high-quality studies (3 studies) (Jia et al., 2010). Mehrabani et al. conducted a meta-analysis on the impact of cocoa consumption on markers of oxidative stress. They reported that malondialdehyde and 8-iso-prostaglandin F2α were significantly reduced, but not in other markers of oxidative stress (Mehrabani et al., 2020).
Consequently, several factors can lead to these controversial results, including different dosages and duration of DC, sample sizes of studies, the diverse status of subjects' health, and initial levels of CRP (Haghighat et al., 2013, Sangsefidi et al., 2020). Also depending on the concentration of dark chocolates' polyphenols and free radical sources, the role of polyphenols could differ between antioxidants and pro-oxidants and subsequently act as either anti-inflammatory or pro-inflammatory compounds (Cao et al., 1997, Di Giuseppe et al., 2008).
The role of inflammation in the pathogenesis of many chronic diseases, such as different cancers diabetes and cardiovascular disease is undeniable (Libby, 2007). On the other hand, many studies represent the protective role of flavonols on the inflammatory pathway (Kuebler et al., 2016, Selmi et al., 2008). The underlying mechanisms by which DC can attenuate inflammatory responses include inhibition of cyclooxygenase-2, prevention of the activation of T-cell and B-cells, reducing the expression and secretion of Interleukin 2, and reducing the amount and properties of inflammatory cytokines (IL5, TNF-α, TGF-β) (Haghighat et al., 2013, Mao et al., 2000, Sanbongi et al., 1997). Possibly DC can mediate these events via transcription factors, such as nuclear transcription factor-kB (NF-kB), affecting the transcription and secretion of many cytokines (Mao et al., 2000).
The advantages of the present study include using advanced search strategies, lack of linguistic restrictions in the search process, quality assessment based on Cochrane criteria, and different subgroup analyses according to duration and dosage of supplementation. However, there are some limitations, including the low quality of the related clinical trials and the significant heterogeneity, resulting from different doses of DC (22-100 g/day), supplemental period (15-56 days), different study size (20-158), and diverse characteristics of participants, such as health status, age, and gender. On the other hand, owing to the high publication bias, caution needs to be considered about the result of this study.
The current study results reveal that the treatment with DC had no significant effect on the CRP level. Due to the controversial finding of the conducted clinical trials, more studies with more quality and bigger sample sizes are required to verify the positive impact of DC in reducing CRP level.
Acknowledgment
Thanks are owed to the Nutrition and Food Security Research Center in Shahid Sadoughi University of Medical Sciences in Yazd, Iran, for supporting this study.
Conflict of interest
The authors declare no conflict of interest.
Funding
There was no role of the funding in the preparation of this study.
Authors’ contributions
Yaghoubi F and Darabi Z prepared the proposal, obtained ethical approvals, applied for
funding and Yaghoubi F, Ahmadi A, Darabi Z and Sangsefidi ZS wrote the manuscript and performed data analysis. Hosseinzadeh M conceived the idea and supervised the study. All authors read and approved the final manuscript.
References
Borenstein M, Hedges LV, Higgins JP & Rothstein HR 2011. Introduction to meta-analysis. John Wiley & Sons.
Cao G, Sofic E & Prior RL 1997. Antioxidant and prooxidant behavior of flavonoids: structure-activity relationships. Free radical biology and medicine. 22 (5): 749-760.
Cottone S, et al. 2006. Relation of C-reactive protein to oxidative stress and to endothelial activation in essential hypertension. American journal of hypertension. 19 (3): 313-318.
da Costa Teixeira AMN, et al. 2017. The impact of dark chocolate intake on arterial elasticity in individuals with HIV/AIDS undergoing ART: a randomized, double-blind, crossover trial. Food & function. 8 (6): 2212-2219.
Desch S, et al. 2010. Low vs. higher-dose dark chocolate and blood pressure in cardiovascular high-risk patients. American journal of hypertension. 23 (6): 694-700.
Di Giuseppe R, et al. 2008. Regular consumption of dark chocolate is associated with low serum concentrations of C-reactive protein in a healthy Italian population. Journal of nutrition. 138 (10): 1939-1945.
Di Renzo L, et al. 2013. Effects of dark chocolate in a population of normal weight obese women:a pilot study. European review for medical and pharmacological sciences. 17 (16): 2257-2266.
Duval S & Tweedie R 2000. Trim and fill: a simple funnel‐plot–based method of testing and adjusting for publication bias in meta‐analysis. Biometrics. 56 (2): 455-463.
Fernández-Real JM & Ricart W 2003. Insulin resistance and chronic cardiovascular inflammatory syndrome. Endocrine reviews. 24 (3): 278-301.
Grassi D, et al. 2008. Blood pressure is reduced and insulin sensitivity increased in glucose-intolerant, hypertensive subjects after 15 days of consuming high-polyphenol dark chocolate. Journal of nutrition. 138 (9): 1671-1676.
Grassi D, et al. 2005. Cocoa reduces blood pressure and insulin resistance and improves endothelium-dependent vasodilation in hypertensives. Hypertension. 46 (2): 398-405.
Haber SL & Gallus K 2012. Effects of dark chocolate on blood pressure in patients with hypertension. American journal of health-system pharmacy. 69 (15): 1287-1288, 1290, 1292-1283.
Haghighat N, et al. 2013. The effects of dark chocolate on lipid profile, apo-lipoprotein A-1, apo-lipoprotein B and inflammation in type-2 diabetic patients: A randomized clinical trial. Iranian journal of nutrition sciences & food technology. 8 (2): 21-30.
Hamed MS, et al. 2008. Dark chocolate effect on platelet activity, C-reactive protein and lipid profile: a pilot study. Southern medical journal. 101 (12): 1203-1208.
Higgins J 2011. GSE Cochrane Handbook for Systematic Systematic Reviews of Interventions Version 5.1. 0.
Higgins J, et al. 2019. Cochrane handbook for systematic reviews of interventions. John Wiley & Sons.
Higgins J & Thompson SG 2002. Quantifying heterogeneity in a meta‐analysis. Statistics in medicine. 21 (11): 1539-1558.
Hooper L, et al. 2012. Effects of chocolate, cocoa, and flavan-3-ols on cardiovascular health: a systematic review and meta-analysis of randomized trials. American journal of clinical nutrition. 95 (3): 740-751.
Hotamisligil GS 2010. Endoplasmic reticulum stress and the inflammatory basis of metabolic disease. Cell. 140 (6): 900-917.
Hotamisligil GS, Shargill NS & Spiegelman BM 1993. Adipose expression of tumor necrosis factor-alpha: direct role in obesity-linked insulin resistance. Science. 259 (5091): 87-91.
Jafarirad S, et al. 2018. Dark chocolate effect on serum adiponectin, biochemical and inflammatory parameters in diabetic patients: A randomized clinical trial. International journal of preventive medicine. 9.
Javadi F, et al. 2017. The effect of quercetin on inflammatory factors and clinical symptoms in women with rheumatoid arthritis: a double-blind, randomized controlled trial. Journal of the American college of nutrition. 36 (1): 9-15.
Jia L, et al. 2010. Short-term effect of cocoa product consumption on lipid profile: a meta-analysis of randomized controlled trials. American journal of clinical of nutrition. 92: 218-225.
Kord-Varkaneh H, Ghaedi E, Nazary-Vanani A, Mohammadi H & Shab-Bidar S 2019. Does cocoa/dark chocolate supplementation have favorable effect on body weight, body mass index and waist circumference? A systematic review, meta-analysis and dose-response
of randomized clinical trials. Critical reviews in food science and nutrition. 59 (15): 2349-2362.
Kuebler U, et al. 2016. Dark chocolate attenuates intracellular pro-inflammatory reactivity to acute psychosocial stress in men: A randomized controlled trial. Brain, behavior, and immunity. 57: 200-208.
Kurlandsky SB & Stote KS 2006. Cardioprotective effects of chocolate and almond consumption in healthy women. Nutrition research. 26 (10): 509-516.
Libby P 2007. Inflammatory mechanisms: the molecular basis of inflammation and disease. Nutrition reviews. 65 (12 Pt 2): S140-146.
Magrone T, Russo MA & Jirillo E 2017. Cocoa and dark chocolate polyphenols: from biology to clinical applications. Frontiers in immunology. 8: 677.
Malhi H & Loomba R 2016. Editorial: dark chocolate may improve NAFLD and metabolic syndrome by reducing oxidative stress. Alimentary pharmacology & therapeutics. 44 (5): 533-534.
Mao T, et al. 2000. Effect of cocoa procyanidins on the secretion of interleukin-4 in peripheral blood mononuclear cells. Journal of medicinal food. 3 (2): 107-114.
Mao T, Water JVD, Keen C, Schmitz H & Gershwin M 2003. Cocoa Flavonols and Procyanidins Promote Transforming Growth Factor-β1 Homeostasis in Peripheral Blood Mononuclear Cells1. Experimental biology and medicine. 228 (1): 93-99.
Mehrabani S, Arab A, Mohammadi H & Amani R 2020. The effect of cocoa consumption on markers of oxidative stress: A systematic review and meta-analysis of interventional studies. Complementary therapies in medicine. 48: 102240.
Mizuno Y, Jacob RF & Mason RP 2011. Inflammation and the development of atherosclerosis: effects of lipid-lowering therapy. Journal of atherosclerosis and thrombosis. 1103160359-1103160359.
Moher D, et al. 2015. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Systematic review. 4 (1): 1.
Montagna MT, et al. 2019. Chocolate,“food of the gods”: History, science, and human health. International journal of environmental research and public health. 16 (24): 4960.
Nahrendorf M & Swirski FK 2015. Neutrophil-macrophage communication in inflammation and atherosclerosis. Science. 349 (6245): 237-238.
Nanetti L, et al. 2012. Effect of consumption of dark chocolate on oxidative stress in lipoproteins and platelets in women and in men. Appetite. 58 (1): 400-405.
Nanetti L, et al. 2008. Effect of consumption of dark chocolate on lipoproteins and serum lipids. Mediterranean journal of nutrition and metabolism. 1 (1): 25.
Ramiro E, et al. 2005. Flavonoids from Theobroma cacao down-regulate inflammatory mediators. Journal of agricultural and food chemistry. 53 (22): 8506-8511.
Rezazadeh A, Mahmoodi M, Mard SA & karimi Moghaddam E 2015. The effects of dark chocolate consumption on lipid profile, fasting blood sugar, liver enzymes, inflammation, and antioxidant status in patients with non-alcoholic fatty liver disease: a randomized, placebo-controlled, pilot study. Journal of gastroenterology and hepatology research. 4 (12): 1858-1864.
Sanbongi C, Suzuki N & Sakane T 1997. Polyphenols in chocolate, which have antioxidant activity, modulate immune functions in humansin vitro. Cellular immunology. 177 (2): 129-136.
Sangsefidi ZS, Yaghoubi F, Hajiahmadi S & Hosseinzadeh M 2020. The effect of coenzyme Q10 supplementation on oxidative stress: A systematic review and meta‐analysis of randomized controlled clinical trials. Food science & nutrition. 8 (4): 1766-1776.
Selmi C, Cocchi CA, Lanfredini M, Keen CL & Gershwin ME 2008. Chocolate at heart: The anti‐inflammatory impact of cocoa flavanols. Molecular nutrition & food research. 52 (11): 1340-1348.
Sudarma V, Sukmaniah S & Siregar P 2011. Effect of dark chocolate on nitric oxide serum levels and blood pressure in prehypertension subjects. Acta medica Indonesiana. 43 (4): 224-228.
Tlaskalová-Hogenová H, et al. 2011. The role of gut microbiota (commensal bacteria) and the mucosal barrier in the pathogenesis of inflammatory and autoimmune diseases and cancer: contribution of germ-free and gnotobiotic animal models of human diseases. Cellular & molecular immunology. 8 (2): 110-120.
Wellen KE & Hotamisligil GS 2005. Inflammation, stress, and diabetes. Journal of clinical investigation. 115 (5): 1111-1119.
Type of article: review article |
Subject:
public specific
Received: 2021/12/2 | Published: 2022/11/19 | ePublished: 2022/11/19
Received: 2021/12/2 | Published: 2022/11/19 | ePublished: 2022/11/19
References
1. Borenstein M, Hedges LV, Higgins JP & Rothstein HR 2011. Introduction to meta-analysis. John Wiley & Sons.
2. Cao G, Sofic E & Prior RL 1997. Antioxidant and prooxidant behavior of flavonoids: structure-activity relationships. Free radical biology and medicine. 22 (5): 749-760.
3. Cottone S, et al. 2006. Relation of C-reactive protein to oxidative stress and to endothelial activation in essential hypertension. American journal of hypertension. 19 (3): 313-318.
4. da Costa Teixeira AMN, et al. 2017. The impact of dark chocolate intake on arterial elasticity in individuals with HIV/AIDS undergoing ART: a randomized, double-blind, crossover trial. Food & function. 8 (6): 2212-2219.
5. Desch S, et al. 2010. Low vs. higher-dose dark chocolate and blood pressure in cardiovascular high-risk patients. American journal of hypertension. 23 (6): 694-700.
6. Di Giuseppe R, et al. 2008. Regular consumption of dark chocolate is associated with low serum concentrations of C-reactive protein in a healthy Italian population. Journal of nutrition. 138 (10): 1939-1945.
7. Di Renzo L, et al. 2013. Effects of dark chocolate in a population of normal weight obese women: a pilot study. European review for medical
9. and pharmacological sciences. 17 (16): 2257-2266.
10. Duval S & Tweedie R 2000. Trim and fill: a simple funnel‐plot–based method of testing and adjusting for publication bias in meta‐analysis. Biometrics. 56 (2): 455-463.
11. Fernández-Real JM & Ricart W 2003. Insulin resistance and chronic cardiovascular inflammatory syndrome. Endocrine reviews. 24 (3): 278-301.
12. Grassi D, et al. 2008. Blood pressure is reduced and insulin sensitivity increased in glucose-intolerant, hypertensive subjects after 15 days of consuming high-polyphenol dark chocolate. Journal of nutrition. 138 (9): 1671-1676.
13. Grassi D, et al. 2005. Cocoa reduces blood pressure and insulin resistance and improves endothelium-dependent vasodilation in hypertensives. Hypertension. 46 (2): 398-405.
14. Haber SL & Gallus K 2012. Effects of dark chocolate on blood pressure in patients with hypertension. American journal of health-system pharmacy. 69 (15): 1287-1288, 1290, 1292-1283.
15. Haghighat N, et al. 2013. The effects of dark chocolate on lipid profile, apo-lipoprotein A-1, apo-lipoprotein B and inflammation in type-2 diabetic patients: A randomized clinical trial. Iranian journal of nutrition sciences & food technology. 8 (2): 21-30.
16. Hamed MS, et al. 2008. Dark chocolate effect on platelet activity, C-reactive protein and lipid profile: a pilot study. Southern medical journal. 101 (12): 1203-1208.
17. Higgins J 2011. GSE Cochrane Handbook for Systematic Systematic Reviews of Interventions Version 5.1. 0.
18. Higgins J, et al. 2019. Cochrane handbook for systematic reviews of interventions. John Wiley & Sons.
19. Higgins J & Thompson SG 2002. Quantifying heterogeneity in a meta‐analysis. Statistics in medicine. 21 (11): 1539-1558.
20. Hooper L, et al. 2012. Effects of chocolate, cocoa, and flavan-3-ols on cardiovascular health: a systematic review and meta-analysis of randomized trials. American journal of clinical nutrition. 95 (3): 740-751.
21. Hotamisligil GS 2010. Endoplasmic reticulum stress and the inflammatory basis of metabolic disease. Cell. 140 (6): 900-917.
22. Hotamisligil GS, Shargill NS & Spiegelman BM 1993. Adipose expression of tumor necrosis factor-alpha: direct role in obesity-linked insulin resistance. Science. 259 (5091): 87-91.
23. Jafarirad S, et al. 2018. Dark chocolate effect on serum adiponectin, biochemical and inflammatory parameters in diabetic patients: A randomized clinical trial. International journal of preventive medicine. 9.
24. Javadi F, et al. 2017. The effect of quercetin on inflammatory factors and clinical symptoms in women with rheumatoid arthritis: a double-blind, randomized controlled trial. Journal of the American college of nutrition. 36 (1): 9-15.
25. Jia L, et al. 2010. Short-term effect of cocoa product consumption on lipid profile: a meta-analysis of randomized controlled trials. American journal of clinical of nutrition. 92: 218-225.
26. Kord-Varkaneh H, Ghaedi E, Nazary-Vanani A, Mohammadi H & Shab-Bidar S 2019. Does cocoa/dark chocolate supplementation have favorable effect on body weight, body mass index and waist circumference? A systematic review, meta-analysis and dose-response of randomized clinical trials. Critical reviews in food science and nutrition. 59 (15): 2349-2362.
27. Kuebler U, et al. 2016. Dark chocolate attenuates intracellular pro-inflammatory reactivity to acute psychosocial stress in men: A randomized controlled trial. Brain, behavior, and immunity. 57: 200-208.
28. Kurlandsky SB & Stote KS 2006. Cardioprotective effects of chocolate and almond consumption in healthy women. Nutrition research. 26 (10): 509-516.
29. Libby P 2007. Inflammatory mechanisms: the molecular basis of inflammation and disease. Nutrition reviews. 65 (12 Pt 2): S140-146.
30. Magrone T, Russo MA & Jirillo E 2017. Cocoa and dark chocolate polyphenols: from biology to clinical applications. Frontiers in immunology. 8: 677.
31. Malhi H & Loomba R 2016. Editorial: dark chocolate may improve NAFLD and metabolic syndrome by reducing oxidative stress. Alimentary pharmacology & therapeutics. 44 (5): 533-534.
32. Mao T, et al. 2000. Effect of cocoa procyanidins on the secretion of interleukin-4 in peripheral blood mononuclear cells. Journal of medicinal food. 3 (2): 107-114.
33. Mao T, Water JVD, Keen C, Schmitz H & Gershwin M 2003. Cocoa Flavonols and Procyanidins Promote Transforming Growth Factor-β1 Homeostasis in Peripheral Blood Mononuclear Cells1. Experimental biology and medicine. 228 (1): 93-99.
34. Mehrabani S, Arab A, Mohammadi H & Amani R 2020. The effect of cocoa consumption on markers of oxidative stress: A systematic review and meta-analysis of interventional studies. Complementary therapies in medicine. 48: 102240.
35. Mizuno Y, Jacob RF & Mason RP 2011. Inflammation and the development of atherosclerosis: effects of lipid-lowering therapy. Journal of atherosclerosis and thrombosis. 1103160359-1103160359.
36. Moher D, et al. 2015. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Systematic review. 4 (1): 1.
37. Montagna MT, et al. 2019. Chocolate,“food of the gods”: History, science, and human health. International journal of environmental research and public health. 16 (24): 4960.
38. Nahrendorf M & Swirski FK 2015. Neutrophil-macrophage communication in inflammation and atherosclerosis. Science. 349 (6245): 237-238.
39. Nanetti L, et al. 2012. Effect of consumption of dark chocolate on oxidative stress in lipoproteins and platelets in women and in men. Appetite. 58 (1): 400-405.
40. Nanetti L, et al. 2008. Effect of consumption of dark chocolate on lipoproteins and serum lipids. Mediterranean journal of nutrition and metabolism. 1 (1): 25.
41. Ramiro E, et al. 2005. Flavonoids from Theobroma cacao down-regulate inflammatory mediators. Journal of agricultural and food chemistry. 53 (22): 8506-8511.
42. Rezazadeh A, Mahmoodi M, Mard SA & karimi Moghaddam E 2015. The effects of dark chocolate consumption on lipid profile, fasting blood sugar, liver enzymes, inflammation, and antioxidant status in patients with non-alcoholic fatty liver disease: a randomized, placebo-controlled, pilot study. Journal of gastroenterology and hepatology research. 4 (12): 1858-1864.
43. Sanbongi C, Suzuki N & Sakane T 1997. Polyphenols in chocolate, which have antioxidant activity, modulate immune functions in humansin vitro. Cellular immunology. 177 (2): 129-136.
44. Sangsefidi ZS, Yaghoubi F, Hajiahmadi S & Hosseinzadeh M 2020. The effect of coenzyme Q10 supplementation on oxidative stress: A systematic review and meta‐analysis of randomized controlled clinical trials. Food science & nutrition. 8 (4): 1766-1776.
45. Selmi C, Cocchi CA, Lanfredini M, Keen CL & Gershwin ME 2008. Chocolate at heart: The anti‐inflammatory impact of cocoa flavanols. Molecular nutrition & food research. 52 (11): 1340-1348.
46. Sudarma V, Sukmaniah S & Siregar P 2011. Effect of dark chocolate on nitric oxide serum levels and blood pressure in prehypertension subjects. Acta medica Indonesiana. 43 (4): 224-228.
47. Tlaskalová-Hogenová H, et al. 2011. The role of gut microbiota (commensal bacteria) and the mucosal barrier in the pathogenesis of inflammatory and autoimmune diseases and cancer: contribution of germ-free and gnotobiotic animal models of human diseases. Cellular & molecular immunology. 8 (2): 110-120.
48. Wellen KE & Hotamisligil GS 2005. Inflammation, stress, and diabetes. Journal of clinical investigation. 115 (5): 1111-1119.
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
