
Sun, May 19, 2024
[Archive]
Volume 8, Issue 4 (Nov 2023)
JNFS 2023, 8(4): 694-708 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Ramezani-Jolfaie N, Khademi Bafrooei M, Lorzadeh E, Javdan G, Razmpour F, Shahab Jahanlou A, et al . Effects of Hesperidin Supplementation on Anthropometric Indices in Adults: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. JNFS 2023; 8 (4) :694-708
URL: http://jnfs.ssu.ac.ir/article-1-606-en.html
URL: http://jnfs.ssu.ac.ir/article-1-606-en.html
Nahid Ramezani-Jolfaie 

 , Mojtaba Khademi Bafrooei , Elnaz Lorzadeh , Gholamali Javdan , Farkhondeh Razmpour , Alireza Shahab Jahanlou , Amin Salehi-Abargouei , Mohammad Mohammadi *
, Mojtaba Khademi Bafrooei , Elnaz Lorzadeh , Gholamali Javdan , Farkhondeh Razmpour , Alireza Shahab Jahanlou , Amin Salehi-Abargouei , Mohammad Mohammadi *
, Mojtaba Khademi Bafrooei , Elnaz Lorzadeh , Gholamali Javdan , Farkhondeh Razmpour , Alireza Shahab Jahanlou , Amin Salehi-Abargouei , Mohammad Mohammadi *
Food Health Research Center, Hormozgan University of Medical Sciences, Bandar Abbas, Iran
Full-Text [PDF 769 kb]
(148 Downloads)
| Abstract (HTML) (1026 Views)
.PNG)
.PNG)
Full-Text: (48 Views)
Effects of Hesperidin Supplementation on Anthropometric Indices in Adults: A Systematic Review and Meta-Analysis of Randomized Controlled Trials
Nahid Ramezani-Jolfaie; PhD1,2, Mojtaba Khademi Bafrooei; PhD3, Elnaz Lorzadeh; MSc4,
Gholamali Javdan; MD, PhD1,2, Farkhondeh Razmpour; PhD1,2, Alireza Shahab Jahanlou; PhD5,
Amin Salehi-Abargouei; PhD6,7 & Mohammad Mohammadi; PhD*1,2
Nahid Ramezani-Jolfaie; PhD1,2, Mojtaba Khademi Bafrooei; PhD3, Elnaz Lorzadeh; MSc4,
Gholamali Javdan; MD, PhD1,2, Farkhondeh Razmpour; PhD1,2, Alireza Shahab Jahanlou; PhD5,
Amin Salehi-Abargouei; PhD6,7 & Mohammad Mohammadi; PhD*1,2
1 Food Health Research Center, Hormozgan University of Medical Sciences, Bandar Abbas, Iran; 2 Department of Community Medicine, School of Medicine, Hormozgan University of Medical Sciences, Bandar Abbas, Iran;
3 Department of Internal Medicine, School of Medicine, Hormozgan University of Medical Sciences, Bandar Abbas, Iran; 4 School of Medicine, Faculty of Science, Medicine and Health, University of Wollongong, Wollongong, NSW 2522, Australia; 5 Cardiovascular Research Center, Hormozgan University of Medical Sciences, Bandar Abbas, Iran;
6 Nutrition and Food Security Research Center, Shahid Sadoughi University of Medical Sciences, Yazd, Iran;
7 Department of Nutrition, School of Public Health, Shahid Sadoughi University of Medical Sciences, Yazd, Iran.
3 Department of Internal Medicine, School of Medicine, Hormozgan University of Medical Sciences, Bandar Abbas, Iran; 4 School of Medicine, Faculty of Science, Medicine and Health, University of Wollongong, Wollongong, NSW 2522, Australia; 5 Cardiovascular Research Center, Hormozgan University of Medical Sciences, Bandar Abbas, Iran;
6 Nutrition and Food Security Research Center, Shahid Sadoughi University of Medical Sciences, Yazd, Iran;
7 Department of Nutrition, School of Public Health, Shahid Sadoughi University of Medical Sciences, Yazd, Iran.
| ARTICLE INFO | ABSTRACT | |
| SYSTEMATIC REVIEW and META_ANALYSIS | Background: Although some studies have reported that flavonoids can be associated with anti-obesity effects, the putative effects of hesperidin, as a subgroup of flavonoids, on anthropometric parameters are inconclusive. Therefore, this systematic review and meta-analysis of randomized controlled trials (RCTs) was conducted to determine the effect of hesperidin supplementation on anthropometric measures in adults. Methods: A comprehensive literature search was performed until February 2022 in electronic databases such as PubMed, Scopus, Web of Science, and Google Scholar. The pooled results were obtained by a random-effects model. Results: A total of nine RCTs enrolling 493 participants were identified. Seven studies had illustrated the effect of hesperidin on weight, eight on body mass index (BMI), five on waist circumference (WC), two on waist to hip ratio (WHR), and two on hip circumference (HC). The results of the pooled analysis showed no significant changes in body weight (0.01 kg, 95% CI: -0.22, 0.24), BMI (-0.02 kg/m2, 95% CI: -0.16, 0.13), and WC (-0.48 cm, 95% CI: -1.52, 0.55) after hesperidin supplementation compared to the control group (P > 0.05). Qualitative assessment of other anthropometric indices also showed no beneficial effect of hesperidin in reducing WHR and HC values; however, these findings are not conclusive because of the limited number of studies. Conclusion: The present study provides no evidence that hesperidin supplementation is effective in improving anthropometric measures. More high-quality RCTs especially among overweight and obese individuals are needed to strengthen the evidence. Keywords: Hesperidin; Body weight; Anthropometry; Systematic review; Meta-analysis |
|
| Article history: Received: 26 Mar 2022 Revised: 8 May 2022 Accepted: 8 Jun 2022 |
||
| *Corresponding author: Mohammadi.nut@gmail.com Department of Community Medicine School of Medicine, Hormozgan University of Medical Sciences, Bandar Abbas, Iran. Postal code: 7919693116 Tel: +98 76 33710373 |
Introduction
As a complex and chronic medical condition, obesity is a worldwide health problem (Thomas et al., 2014) and it is a cluster of complications such as impaired glucose tolerance, dyslipidemia, hypertension, and systemic inflammation (Stoner and Cornwall, 2014). It is also a leading cause of extensive morbidity and mortality with a high economic burden in both developing and developed nations (Lehnert et al., 2013, Ng et al., 2014). Obesity is one of the direct sources for progression or occurrence of various diseases such as cardiovascular diseases (Mandviwala et al., 2016), insulin resistance and diabetes (Genser et al., 2016), non-alcoholic fatty liver disease (Li et al., 2016), gallstone disease and pancreatitis (Bonfrate et al., 2014), esophageal reflux (Khan et al., 2016), inflammatory bowel disease (Harper and Zisman, 2016), chronic kidney disease (Briffa et al., 2013), poly ovary syndrome (Orio et al., 2016), neurological diseases (Martin-Jiménez et al., 2017), and different types of cancer (Donohoe et al., 2017). It has been reported that the prevalence of overweight and obesity has been growing from 29% to 38% in the past three decades (Ng et al., 2014). Recent reports from World Health Organization in 2016 have suggested that 1.9 billion people are overweight, of whom 650 million are considered to be obese (World Health Organization, October 2017).
Different weight management strategies have been used throughout the years, including dietary regimen approaches or dietary constituents with anti-obesity potentials (Tuomilehto et al., 2001). However, some of the traditional recommendations have been proved to be impractical and disappointing due to poor attendance and adherence rates (Butryn et al., 2011, Huisman et al., 2010, Zuckoff, 2012). Thus, novel strategies are desperately needed to be suggested as more effective ways to get rid of excessive fat (Soeliman and Azadbakht, 2014). A variety of weight loss supplements sold under the title of “slimming aids” is already available although the outcome of each remains uncertain (Derosa and Maffioli, 2012, Mousavi et al., 2018, Onakpoya et al., 2011). It has been demonstrated that dietary intake of a widespread group of plant polyphenols known as flavonoids can exert anti-obesity effects; however, enough evidence is not available in this regard (Bertoia et al., 2016). Some trials suggest that a potential effect of polyphenols can reduce body weight by increasing energy expenditure (Barth et al., 2012, Dallas et al., 2014, Most et al., 2014) even though other findings have shown null or contrasting results (Bell et al., 2011, Janssens et al., 2015).
Hesperidin is a flavonone glycoside that along with narirutin is a subgroup of flavonoids that mainly exist in the solid parts of citrus fruits and the membranes separating the pulp segments; this explains why the concentration of these flavonones is higher in whole-fruit juices (Roowi et al., 2009). There is evidence on the cardio-protective effects and anti-inflammatory properties of hesperidin (Amiot et al., 2016, Lorzadeh et al., 2019, Mulvihill et al., 2016). However, some of these results are inconsistent with recent meta-analyses suggesting hesperidin supplementation might not have any impact on lipid profile, blood pressure, and blood glucose control (Mohammadi et al., 2019, Shams-Rad et al., 2020). Although there is still no strong evidence on the association between flavanones and weight loss, some studies have investigated hesperidin as a supplement for obesity management and reported that it may be useful for the prevention or treatment of obesity (Ohara et al., 2016). However, several other studies have not supported these claims (Demonty et al., 2010, Ribeiro et al., 2017, Simpson et al., 2016) . Therefore, this study aims to summarize the available data of randomized controlled clinical trials (RCTs) investigating the effect of hesperidin supplementation on anthropometric parameters in adults.
Materials and Methods
The preferred reporting items of systematic reviews and meta-analysis (PRISMA) statement was followed to design perform and report this systematic review and meta-analysis (Shamseer et al., 2015).
Data sources and search strategy: Medline/Pubmed, Scopus, Web of Science, and Google Scholar were systematically searched from the earliest available online indexing through February 2022. The search was limited to human studies, additionally, no language restriction was performed. Two investigators (Ramezani-Jolfaie N and Mohammadi M) independently assessed the relevancy of studies by their title and abstracts as well as full text if needed in the next step. Additionally, the references of selected articles were examined manually for any missing related studies. Three groups of medical subject heading terms (MeSH) and non-MeSH keywords were used in constructing the database search as follows: group 1: “hesperidin”, “hesperitin”, “citrus flavonoid”, “orange juice”; group 2: “intervention”, “trial”, “randomized”, “random”, “randomly”, “placebo”, “assignment”, “clinical trial”, “RCT”, “cross-over”, “parallel”, “body weight”, weight, “body mass index”, BMI, “waist circumference”, WC, “waist-hip ratio”, WHR, “hip circumference”, HC, “fat free mass”, FFM, “fat mass”, FM, “lean body mass”, LBM; group 3: “mouse”, “mice”, “rats”, “in vitro”, “pig”, “rabbit”, “rooster”, “cell”, “cow” that combined by utilizing the “NOT” Boolean operator.
Selection criteria: The Population, Intervention, Comparison, Outcome, and Study types (PICOS) are provided in Table 1. The original RCTs were considered for inclusion if they had supplemented hesperidin in human adults. Studies were excluded if they had a short duration of intervention (lower than 2 weeks), were conducted among children/adolescents below 18 years of age, and if they had no control/placebo comparison group or outcomes of interest or reported duplicate data. Studies with interventions containing the other components in addition to the hesperidin were also excluded.
Data extraction: Study details were extracted and recorded independently by two authors (Ramezani-Jolfaie N and Mohammadi M) and in case of any disagreement, a third party (Salehi-Abargouei A) was consulted to reach mutual consensus. The following information of the included RCTs was collected: study design (crossover or parallel), ethnic or country, the last name of each author, year of article publication, subject baseline characteristics (sample size, gender, age, and overall health status), intervention duration, the use of run-in or washout periods, dose of hesperidin intake (mg/day), type of intervention used in the control groups, and the number of participants who completed the follow-up period.
Risk of bias assessment: Risk of bias assessment was conducted against the following key criteria according to the recommendation of the Cochrane Collaboration (Higgins and Green, 2011): random sequence generation; allocation concealment; blinding of participants, personnel and assessors; incomplete outcome data; selective outcome reporting and other sources of bias. Determination of bias level was either low (proper methods taken to reduce bias), high (improper methods resulting in bias), or unclear (either a lack of sufficient information or uncertainty over a potential bias) risk of bias. Six domains were presented as the (‘key domains’) and used to decide whether each RCT was low risk (low for all key domains), high risk (high for one or more key domains), and unclear risk (unclear for at most one or more key domains). Any discrepancies were resolved by consulting with a third author if necessary (ASA).
Data analysis: The mean change values with their respective standard deviations (SDs) between baseline and end of the study in both treatment and control groups were extracted. If change values were not reported by the studies, the baseline and final mean values with their respective SDs were used to calculate the mean±SD of changes in outcomes by a correlation coefficient of 0.5. Further analyses using r = 0.1 and 0.9 were also performed to check the sensitivity of the findings to the selected correlation coefficient. The random-effects model was used to examine the weighted mean differences (WMDs) and 95% confidence intervals (CIs). To assess the between-study heterogeneity, I2 statistics and Chi-square were incorporated which considered as significant and high by P-values < 0.05 for Chi-square and I2 values of more than 50%, respectively. Subgroups analysis was performed according to intervention duration (<8 weeks or >=8 weeks), dosage of hesperidin (<= 500 mg/day or > 500 mg/day), and health status of individuals (cardio-metabolic disorders or healthy) to explore the potential sources of heterogeneity. To test the robustness of the meta-analysis results, sensitivity analysis was also conducted by removing one trial at a time and recalculating the overall effects with the remaining studies. Moreover, the visual inspection of the funnel plots represented the possibility of publication bias (Egger et al., 2008). All the analyses were done by STATA software version 13.0 (StataCorp, Texas, USA) for which p-values less than 0.05 were considered statistically significant.
Results
Search results
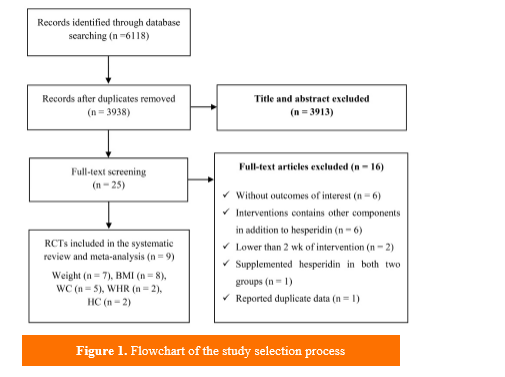
In general, out of 6118 published articles that initially identified through systematic data search, 2180 were detected as duplicates and 3913 were excluded after title and abstract screening for not meeting the inclusion criteria. A total of 25 articles remained for full text evaluation from which 16 articles were further excluded for the following reasons: (i) did not report the outcomes of interest (n=6) (Cheraghpour et al., 2019, Kean et al., 2015, Martínez-Noguera et al., 2020, Milenkovic et al., 2011, Salden et al., 2016), (ii) had interventions containing other components in addition to hesperidin (n=6) (Rangel-Huerta et al., 2015, Valls et al., 2021a, Valls et al., 2021b, Yari et al., 2021c, Yoshitomi et al., 2021), (iii) had a short duration of intervention (<2 weeks, n=2) (Lamport et al., 2016, Schär et al., 2015), (iv) had no suitable control group (n=1) (Miwa et al., 2004), (v) reported duplicate data (n=1) (Homayouni et al., 2018). Nine studies were finally included in the present systematic review and meta-analysis (Demonty et al., 2010, Eghtesadi et al., 2016, Haidari et al., 2015, Homayouni et al., 2017, Ohara et al., 2016, Rizza et al., 2011, Yari et al., 2021a, Yari et al., 2021b, Yari et al., 2019). Seven out of nine articles have reported data on body weight (Demonty et al., 2010, Eghtesadi et al., 2016, Haidari et al., 2015, Homayouni et al., 2017, Ohara et al., 2016, Yari et al., 2021b, Yari et al., 2019), eight on BMI (Demonty et al., 2010, Eghtesadi et al., 2016, Haidari et al., 2015, Homayouni et al., 2017, Ohara et al., 2016, Rizza et al., 2011, Yari et al., 2021a, Yari et al., 2021b), five on waist circumference (WC) (Haidari et al., 2015, Ohara et al., 2016, Rizza et al., 2011, Yari et al., 2021a, Yari et al., 2019), two on hip circumference (HC) (Haidari et al., 2015, Ohara et al., 2016), and two on waist to hip ratio (WHR) (Haidari et al., 2015, Yari et al., 2021a) (Figure 1).
Study characteristics
The basic characteristics of RCTs are presented in Table 2. Nine randomized trials published from 2010 to 2020 were included, 8 of which had a parallel design and one was a cross-over trial (Rizza et al., 2011). Nine studies included 493 participants and sample sizes ranged from 24 to 124 participants of both sexes, aged between 18 to 75 years. The treatment duration lasted for 3 to 12 weeks and the dosage of hesperidin oral administration varied from 500 mg/day to 1000 mg/day. The majority of studies have been conducted in Iran, but one was based in Netherland (Demonty et al., 2010), one in Italy (Rizza et al., 2011), and another one in Japan (Ohara et al., 2016). The participants were either healthy with moderate obesity (Ohara et al., 2016) and moderate hypercholesterolemia (Demonty et al., 2010) or patients with a medical condition such as metabolic syndrome, myocardial infarction, diabetes, and non-alcoholic fatty liver diseases.
Risk of bias assessment: The risk of bias assessment of each RCT is provided in Table 3. Four studies out of nine used an adequate random sequence generator and had a low risk of bias for this domain (Haidari et al., 2015, Homayouni et al., 2017, Yari et al., 2021a, Yari et al., 2019), whereas the remaining five studies had an unclear risk of bias since no detailed method was suggested for randomization (Demonty et al., 2010, Eghtesadi et al., 2016, Ohara et al., 2016, Rizza et al., 2011, Yari et al., 2021b). Only one study by Homayouni et al. (Homayouni et al., 2017) applied adequate allocation concealment and other articles did not report clear data on allocation concealment, hence considered as unclear risk of bias. Two studies were categorized as high risk of bias for blinding of the participants and personnel (Yari et al., 2021a, Yari et al., 2021b); however, by providing enough information about blinding in the remaining studies, they were labeled as low risk of bias. There was no sufficient report on blinding of outcome assessment in any of the included studies. The risk of bias from incomplete outcome data was assessed as low in the majority of the articles except for two (Haidari et al., 2015, Rizza et al., 2011). Regarding selective outcome reporting, all the studies were judged as low risk of bias. As a result, in overall risk of bias, seven of the included studies were assessed as “unclear”, since each study had an unclear risk of bias for at least one of the six domains. Two remaining trials were regarded as “high” risk of bias due to having at least one high-risk domain.
Systematic review
Effect of hesperidin supplementation on HC and WHR: Two studies (n = 104 participants) on HC (Haidari et al., 2015, Ohara et al., 2016) and two studies (n = 118 participants) on WHR (Haidari et al., 2015, Yari et al., 2021a) provided no evidence for the effectiveness of hesperidin in reducing HC and WHR values. Haidari et al. (Haidari et al., 2015) reported no significant differences in HC and WHR at baseline and at the end of the study between hesperidin and placebo groups (P > 0.05). Ohara et al. (Ohara et al., 2016) also showed no significant differences in reducing HC between subjects receiving placebo and those who ingested glucosyl hesperidin with or without caffeine. In a study by Yari et al. (Yari et al., 2021a), hesperidin supplementation also resulted no significant changes in WHR compared to control groups.
Meta-analysis
Effect of hesperidin supplementation on body weight: As provided in Table 4, the pooled estimated effect size of seven studies with 426 participants (Demonty et al., 2010, Eghtesadi et al., 2016, Haidari et al., 2015, Homayouni et al., 2017, Ohara et al., 2016, Yari et al., 2021b, Yari et al., 2019) showed no significant changes in body weight after hesperidin consumption compared to control groups (WMD=0.01 kg, 95% CI: -0.22, 0.24, P=0.918; Figure 2). There was no significant between-study heterogeneity (Q statistics=3.54, P=0.739, I2=0%). We also performed some subgroup analyses to identify the possible different effects of hesperidin supplementation caused by duration and dosage of treatment and health status of the participants; however, no significant changes in weight status were observed in any of the subgroups.
Effect of hesperidin supplementation on BMI: Eight studies with 444 participants were assessed for effects of hesperidin on BMI (Demonty et al., 2010, Eghtesadi et al., 2016, Haidari et al., 2015, Homayouni et al., 2017, Ohara et al., 2016, Rizza et al., 2011, Yari et al., 2021a, Yari et al., 2021b). Hesperidin supplementation was found to have no significant effect on BMI in comparison with control groups (WMD=-0.02 kg/m2, 95% CI: -0.16, 0.13, P=0.831; Figure 3). There was moderate between-study heterogeneity, but it was not significant (Q statistics=9.58, P=0.214, I2 =26.9%). No statistical difference was observed in subgroups according to duration and dosage of treatment and health status of the participants (Table 4).
Effect of hesperidin supplementation on WC: The overall effects of 5 studies including a total of 220 participants (Haidari et al., 2015, Ohara et al., 2016, Rizza et al., 2011, Yari et al., 2021a, Yari et al., 2019) suggested no significant change in WC after hesperidin supplementation compared to control groups (WMD=-0.48 cm, 95% CI: -1.52, 0.55, P=0.362; Figure 4). A significant between-study heterogeneity was found (Q statistics=9.76, P=0.045, I2=59%). When the subgroup analysis was performed based on duration and dosage of treatment, heterogeneity was attenuated and non-significant in their categories; however, no significant change in WC was observed in any of the subgroups (Table 4).
Meta-regression
To examine the possible association of different effects of hesperidin with supplementation dose and study duration on body weight, the meta-regression analysis was performed, but no significant relationship was detected.
Publication bias and sensitivity analysis
The pooled effects of hesperidin intake on weight, BMI, and WC were not sensitive to any of the studies after omitting each out of analyses, suggesting the results were robust. Furthermore, correlation coefficients opted to examine the value changes in the meta-analyses revealed no indication regarding sensitivity.
No publication bias was perceived in the funnel plots and they proved to be symmetrical after considering Begg’s and Egger’s asymmetry tests: weight (Begg’s test, P=0.133; Egger’s test, P=0.027), BMI (Begg’s test, P=0.266; Egger’s test, P=0.062), WC (Begg’s test, P=0.086; Egger’s test, P=0.051).
Different weight management strategies have been used throughout the years, including dietary regimen approaches or dietary constituents with anti-obesity potentials (Tuomilehto et al., 2001). However, some of the traditional recommendations have been proved to be impractical and disappointing due to poor attendance and adherence rates (Butryn et al., 2011, Huisman et al., 2010, Zuckoff, 2012). Thus, novel strategies are desperately needed to be suggested as more effective ways to get rid of excessive fat (Soeliman and Azadbakht, 2014). A variety of weight loss supplements sold under the title of “slimming aids” is already available although the outcome of each remains uncertain (Derosa and Maffioli, 2012, Mousavi et al., 2018, Onakpoya et al., 2011). It has been demonstrated that dietary intake of a widespread group of plant polyphenols known as flavonoids can exert anti-obesity effects; however, enough evidence is not available in this regard (Bertoia et al., 2016). Some trials suggest that a potential effect of polyphenols can reduce body weight by increasing energy expenditure (Barth et al., 2012, Dallas et al., 2014, Most et al., 2014) even though other findings have shown null or contrasting results (Bell et al., 2011, Janssens et al., 2015).
Hesperidin is a flavonone glycoside that along with narirutin is a subgroup of flavonoids that mainly exist in the solid parts of citrus fruits and the membranes separating the pulp segments; this explains why the concentration of these flavonones is higher in whole-fruit juices (Roowi et al., 2009). There is evidence on the cardio-protective effects and anti-inflammatory properties of hesperidin (Amiot et al., 2016, Lorzadeh et al., 2019, Mulvihill et al., 2016). However, some of these results are inconsistent with recent meta-analyses suggesting hesperidin supplementation might not have any impact on lipid profile, blood pressure, and blood glucose control (Mohammadi et al., 2019, Shams-Rad et al., 2020). Although there is still no strong evidence on the association between flavanones and weight loss, some studies have investigated hesperidin as a supplement for obesity management and reported that it may be useful for the prevention or treatment of obesity (Ohara et al., 2016). However, several other studies have not supported these claims (Demonty et al., 2010, Ribeiro et al., 2017, Simpson et al., 2016) . Therefore, this study aims to summarize the available data of randomized controlled clinical trials (RCTs) investigating the effect of hesperidin supplementation on anthropometric parameters in adults.
Materials and Methods
The preferred reporting items of systematic reviews and meta-analysis (PRISMA) statement was followed to design perform and report this systematic review and meta-analysis (Shamseer et al., 2015).
Data sources and search strategy: Medline/Pubmed, Scopus, Web of Science, and Google Scholar were systematically searched from the earliest available online indexing through February 2022. The search was limited to human studies, additionally, no language restriction was performed. Two investigators (Ramezani-Jolfaie N and Mohammadi M) independently assessed the relevancy of studies by their title and abstracts as well as full text if needed in the next step. Additionally, the references of selected articles were examined manually for any missing related studies. Three groups of medical subject heading terms (MeSH) and non-MeSH keywords were used in constructing the database search as follows: group 1: “hesperidin”, “hesperitin”, “citrus flavonoid”, “orange juice”; group 2: “intervention”, “trial”, “randomized”, “random”, “randomly”, “placebo”, “assignment”, “clinical trial”, “RCT”, “cross-over”, “parallel”, “body weight”, weight, “body mass index”, BMI, “waist circumference”, WC, “waist-hip ratio”, WHR, “hip circumference”, HC, “fat free mass”, FFM, “fat mass”, FM, “lean body mass”, LBM; group 3: “mouse”, “mice”, “rats”, “in vitro”, “pig”, “rabbit”, “rooster”, “cell”, “cow” that combined by utilizing the “NOT” Boolean operator.
Selection criteria: The Population, Intervention, Comparison, Outcome, and Study types (PICOS) are provided in Table 1. The original RCTs were considered for inclusion if they had supplemented hesperidin in human adults. Studies were excluded if they had a short duration of intervention (lower than 2 weeks), were conducted among children/adolescents below 18 years of age, and if they had no control/placebo comparison group or outcomes of interest or reported duplicate data. Studies with interventions containing the other components in addition to the hesperidin were also excluded.
Data extraction: Study details were extracted and recorded independently by two authors (Ramezani-Jolfaie N and Mohammadi M) and in case of any disagreement, a third party (Salehi-Abargouei A) was consulted to reach mutual consensus. The following information of the included RCTs was collected: study design (crossover or parallel), ethnic or country, the last name of each author, year of article publication, subject baseline characteristics (sample size, gender, age, and overall health status), intervention duration, the use of run-in or washout periods, dose of hesperidin intake (mg/day), type of intervention used in the control groups, and the number of participants who completed the follow-up period.
Risk of bias assessment: Risk of bias assessment was conducted against the following key criteria according to the recommendation of the Cochrane Collaboration (Higgins and Green, 2011): random sequence generation; allocation concealment; blinding of participants, personnel and assessors; incomplete outcome data; selective outcome reporting and other sources of bias. Determination of bias level was either low (proper methods taken to reduce bias), high (improper methods resulting in bias), or unclear (either a lack of sufficient information or uncertainty over a potential bias) risk of bias. Six domains were presented as the (‘key domains’) and used to decide whether each RCT was low risk (low for all key domains), high risk (high for one or more key domains), and unclear risk (unclear for at most one or more key domains). Any discrepancies were resolved by consulting with a third author if necessary (ASA).
Data analysis: The mean change values with their respective standard deviations (SDs) between baseline and end of the study in both treatment and control groups were extracted. If change values were not reported by the studies, the baseline and final mean values with their respective SDs were used to calculate the mean±SD of changes in outcomes by a correlation coefficient of 0.5. Further analyses using r = 0.1 and 0.9 were also performed to check the sensitivity of the findings to the selected correlation coefficient. The random-effects model was used to examine the weighted mean differences (WMDs) and 95% confidence intervals (CIs). To assess the between-study heterogeneity, I2 statistics and Chi-square were incorporated which considered as significant and high by P-values < 0.05 for Chi-square and I2 values of more than 50%, respectively. Subgroups analysis was performed according to intervention duration (<8 weeks or >=8 weeks), dosage of hesperidin (<= 500 mg/day or > 500 mg/day), and health status of individuals (cardio-metabolic disorders or healthy) to explore the potential sources of heterogeneity. To test the robustness of the meta-analysis results, sensitivity analysis was also conducted by removing one trial at a time and recalculating the overall effects with the remaining studies. Moreover, the visual inspection of the funnel plots represented the possibility of publication bias (Egger et al., 2008). All the analyses were done by STATA software version 13.0 (StataCorp, Texas, USA) for which p-values less than 0.05 were considered statistically significant.
Results
Search results
In general, out of 6118 published articles that initially identified through systematic data search, 2180 were detected as duplicates and 3913 were excluded after title and abstract screening for not meeting the inclusion criteria. A total of 25 articles remained for full text evaluation from which 16 articles were further excluded for the following reasons: (i) did not report the outcomes of interest (n=6) (Cheraghpour et al., 2019, Kean et al., 2015, Martínez-Noguera et al., 2020, Milenkovic et al., 2011, Salden et al., 2016), (ii) had interventions containing other components in addition to hesperidin (n=6) (Rangel-Huerta et al., 2015, Valls et al., 2021a, Valls et al., 2021b, Yari et al., 2021c, Yoshitomi et al., 2021), (iii) had a short duration of intervention (<2 weeks, n=2) (Lamport et al., 2016, Schär et al., 2015), (iv) had no suitable control group (n=1) (Miwa et al., 2004), (v) reported duplicate data (n=1) (Homayouni et al., 2018). Nine studies were finally included in the present systematic review and meta-analysis (Demonty et al., 2010, Eghtesadi et al., 2016, Haidari et al., 2015, Homayouni et al., 2017, Ohara et al., 2016, Rizza et al., 2011, Yari et al., 2021a, Yari et al., 2021b, Yari et al., 2019). Seven out of nine articles have reported data on body weight (Demonty et al., 2010, Eghtesadi et al., 2016, Haidari et al., 2015, Homayouni et al., 2017, Ohara et al., 2016, Yari et al., 2021b, Yari et al., 2019), eight on BMI (Demonty et al., 2010, Eghtesadi et al., 2016, Haidari et al., 2015, Homayouni et al., 2017, Ohara et al., 2016, Rizza et al., 2011, Yari et al., 2021a, Yari et al., 2021b), five on waist circumference (WC) (Haidari et al., 2015, Ohara et al., 2016, Rizza et al., 2011, Yari et al., 2021a, Yari et al., 2019), two on hip circumference (HC) (Haidari et al., 2015, Ohara et al., 2016), and two on waist to hip ratio (WHR) (Haidari et al., 2015, Yari et al., 2021a) (Figure 1).
Study characteristics
The basic characteristics of RCTs are presented in Table 2. Nine randomized trials published from 2010 to 2020 were included, 8 of which had a parallel design and one was a cross-over trial (Rizza et al., 2011). Nine studies included 493 participants and sample sizes ranged from 24 to 124 participants of both sexes, aged between 18 to 75 years. The treatment duration lasted for 3 to 12 weeks and the dosage of hesperidin oral administration varied from 500 mg/day to 1000 mg/day. The majority of studies have been conducted in Iran, but one was based in Netherland (Demonty et al., 2010), one in Italy (Rizza et al., 2011), and another one in Japan (Ohara et al., 2016). The participants were either healthy with moderate obesity (Ohara et al., 2016) and moderate hypercholesterolemia (Demonty et al., 2010) or patients with a medical condition such as metabolic syndrome, myocardial infarction, diabetes, and non-alcoholic fatty liver diseases.
Risk of bias assessment: The risk of bias assessment of each RCT is provided in Table 3. Four studies out of nine used an adequate random sequence generator and had a low risk of bias for this domain (Haidari et al., 2015, Homayouni et al., 2017, Yari et al., 2021a, Yari et al., 2019), whereas the remaining five studies had an unclear risk of bias since no detailed method was suggested for randomization (Demonty et al., 2010, Eghtesadi et al., 2016, Ohara et al., 2016, Rizza et al., 2011, Yari et al., 2021b). Only one study by Homayouni et al. (Homayouni et al., 2017) applied adequate allocation concealment and other articles did not report clear data on allocation concealment, hence considered as unclear risk of bias. Two studies were categorized as high risk of bias for blinding of the participants and personnel (Yari et al., 2021a, Yari et al., 2021b); however, by providing enough information about blinding in the remaining studies, they were labeled as low risk of bias. There was no sufficient report on blinding of outcome assessment in any of the included studies. The risk of bias from incomplete outcome data was assessed as low in the majority of the articles except for two (Haidari et al., 2015, Rizza et al., 2011). Regarding selective outcome reporting, all the studies were judged as low risk of bias. As a result, in overall risk of bias, seven of the included studies were assessed as “unclear”, since each study had an unclear risk of bias for at least one of the six domains. Two remaining trials were regarded as “high” risk of bias due to having at least one high-risk domain.
Systematic review
Effect of hesperidin supplementation on HC and WHR: Two studies (n = 104 participants) on HC (Haidari et al., 2015, Ohara et al., 2016) and two studies (n = 118 participants) on WHR (Haidari et al., 2015, Yari et al., 2021a) provided no evidence for the effectiveness of hesperidin in reducing HC and WHR values. Haidari et al. (Haidari et al., 2015) reported no significant differences in HC and WHR at baseline and at the end of the study between hesperidin and placebo groups (P > 0.05). Ohara et al. (Ohara et al., 2016) also showed no significant differences in reducing HC between subjects receiving placebo and those who ingested glucosyl hesperidin with or without caffeine. In a study by Yari et al. (Yari et al., 2021a), hesperidin supplementation also resulted no significant changes in WHR compared to control groups.
Meta-analysis
Effect of hesperidin supplementation on body weight: As provided in Table 4, the pooled estimated effect size of seven studies with 426 participants (Demonty et al., 2010, Eghtesadi et al., 2016, Haidari et al., 2015, Homayouni et al., 2017, Ohara et al., 2016, Yari et al., 2021b, Yari et al., 2019) showed no significant changes in body weight after hesperidin consumption compared to control groups (WMD=0.01 kg, 95% CI: -0.22, 0.24, P=0.918; Figure 2). There was no significant between-study heterogeneity (Q statistics=3.54, P=0.739, I2=0%). We also performed some subgroup analyses to identify the possible different effects of hesperidin supplementation caused by duration and dosage of treatment and health status of the participants; however, no significant changes in weight status were observed in any of the subgroups.
Effect of hesperidin supplementation on BMI: Eight studies with 444 participants were assessed for effects of hesperidin on BMI (Demonty et al., 2010, Eghtesadi et al., 2016, Haidari et al., 2015, Homayouni et al., 2017, Ohara et al., 2016, Rizza et al., 2011, Yari et al., 2021a, Yari et al., 2021b). Hesperidin supplementation was found to have no significant effect on BMI in comparison with control groups (WMD=-0.02 kg/m2, 95% CI: -0.16, 0.13, P=0.831; Figure 3). There was moderate between-study heterogeneity, but it was not significant (Q statistics=9.58, P=0.214, I2 =26.9%). No statistical difference was observed in subgroups according to duration and dosage of treatment and health status of the participants (Table 4).
Effect of hesperidin supplementation on WC: The overall effects of 5 studies including a total of 220 participants (Haidari et al., 2015, Ohara et al., 2016, Rizza et al., 2011, Yari et al., 2021a, Yari et al., 2019) suggested no significant change in WC after hesperidin supplementation compared to control groups (WMD=-0.48 cm, 95% CI: -1.52, 0.55, P=0.362; Figure 4). A significant between-study heterogeneity was found (Q statistics=9.76, P=0.045, I2=59%). When the subgroup analysis was performed based on duration and dosage of treatment, heterogeneity was attenuated and non-significant in their categories; however, no significant change in WC was observed in any of the subgroups (Table 4).
Meta-regression
To examine the possible association of different effects of hesperidin with supplementation dose and study duration on body weight, the meta-regression analysis was performed, but no significant relationship was detected.
Publication bias and sensitivity analysis
The pooled effects of hesperidin intake on weight, BMI, and WC were not sensitive to any of the studies after omitting each out of analyses, suggesting the results were robust. Furthermore, correlation coefficients opted to examine the value changes in the meta-analyses revealed no indication regarding sensitivity.
No publication bias was perceived in the funnel plots and they proved to be symmetrical after considering Begg’s and Egger’s asymmetry tests: weight (Begg’s test, P=0.133; Egger’s test, P=0.027), BMI (Begg’s test, P=0.266; Egger’s test, P=0.062), WC (Begg’s test, P=0.086; Egger’s test, P=0.051).
| Table 1. The Population, Intervention, Comparison, Outcome, Study types (PICOS) criteria. | |
| Criteria | Description |
| Population | Adults aged >18 year |
| Intervention | Hesperidin supplementation |
| Comparison | Placebo capsule (cellulose, starch) or without treatment |
| Outcome | Weight, body mass index, Waist circumference, Hip circumference, and Waist to hip ratio |
| Study types | Randomized clinical trials |
| Table 2. Characteristics of randomized clinical trials included in the systematic review | |||||||||
| Study, Year (reference) | Country | Number, Sex (F/M) | Age (year) | RCT design | Duration (weeks) | Intervention group | Control group | Reported outcomes | Notes about participants |
| Demonty et al. 2010 (Demonty et al., 2010) |
Netherland | 124 (59F/65M) |
18-75 Int1: 61 Con1:60.1 |
Parallel | 4 | 800 mg/day hesperidin |
800 mg/day placebo (cellulose) |
Weight BMI |
Apparently healthy subjects with moderate hypercholesterolemia |
| Rizza et al. 2011 (Rizza et al., 2011) |
Italy | 24 (9F/15M) |
21-65 Int: 53 Con: 50 |
Cross-over | 3 | 500 mg/day hesperidin |
500 mg/day placebo (cellulose) |
BMI WC |
Patients with metabolic syndrome |
| Haidari et al. 2015 (Haidari et al., 2015) |
Iran | 75 (22F/53M) | 40-65 | Parallel | 4 | 600 mg/day hesperidin |
600 mg/day placebo (starch) |
Weight BMI WC, HC WHR |
Patients with myocardial infarction |
| Ohara et al. 2016 (Ohara et al., 2016) |
Japan | 29 (15F/14M) |
20-65 Int: 49 Con: 49.4 |
Parallel | 12 | 500 mg/day hesperidin |
Placebo | Weight BMI WC, HC |
Healthy moderately obese individuals |
| Eghtesadi et al. 2016 (Eghtesadi et al., 2016) |
Iran | 45 23F/22M |
Int: 53.2 Con:53.4 |
Parallel | 8 | 500 mg/day hesperidin |
500 mg/day placebo (cellulose) |
Weight BMI |
Patients with diabetes |
| Homayouni et al. 2017 (Homayouni et al., 2017) | Iran | 60 (32F/28M) |
30-65 Int: 51.2 Con: 54.4 |
Parallel | 6 | 500 mg/day hesperidin |
500 mg/day placebo (starch) |
Weight BMI |
Patients with diabetes |
| Yari et al. 2019 (Yari et al., 2019) |
Iran | 49 (24F/25M) |
27-70 Int: 45.05 Con: 45.33 |
Parallel | 12 | 1000 mg/day hesperidin |
1000 mg/day placebo (starch) |
Weight WC |
Patients with metabolic syndrome |
| Yari et al. 2021 (Yari et al., 2021b) |
Iran | 44 (21F/23M) |
18-70 Int: 45.82 Con: 46.41 |
Parallel | 12 | 1000 mg/day hesperidin + lifestyle modification program |
lifestyle modification program | Weight BMI |
Patients with metabolic syndrome |
| Yari et al. 2021 (Yari et al., 2021a) |
Iran | 43 ( F/21M) |
18-70 Int: 45.82 Con: 46.11 |
Parallel | 12 | 1000 mg/day hesperidin + lifestyle modification program |
lifestyle modification program | BMI WC WHR |
Patients with non-alcoholic fatty liver disease |
| Table 3. Risk of bias assessment according to the Cochrane collaboration’s risk of bias assessment tool. | |||||||
| Study, year | Random sequence generation | Allocation concealment | Blinding of participants and personnel | Blinding of outcome assessment | Incomplete outcome data | Selective reporting | Overall risk of bias |
| Homayouni et al. 2018 | Low | Low | Low | Unclear | Low | Low | Unclear |
| Ohara et al. 2016 | Unclear | Unclear | Low | Unclear | Low | Low | Unclear |
| Haidari et al. 2015 | Low | Unclear | Low | Unclear | Unclear | Low | Unclear |
| Rizza et al. 2011 | Unclear | Unclear | Low | Unclear | Unclear | Low | Unclear |
| Demonty et al. 2010 | Unclear | Unclear | Low | Unclear | Low | Low | Unclear |
| Eghtesadi et al. 2016 | Unclear | Unclear | Low | Unclear | Low | Low | Unclear |
| Yari et al. 2019 | Low | Unclear | Low | Unclear | Low | Low | Unclear |
| Yari et al. 2021 | Unclear | Unclear | High | Unclear | Low | Low | High |
| Yari et al. 2021 | Low | Unclear | High | Unclear | Low | Low | High |
| Table 4. Effect of hesperidin supplementation on weight and BMI based on several subgroups as well as all studies (all analyses were conducted using random effects model). | ||||||
| Variables | Meta-analysis | Heterogeneity | ||||
| No. of studies |
WMD (95%CI) |
P effect |
Q statistic |
P within group |
I2 (%) | |
| Weight (kg) | ||||||
| Duration of intervention | ||||||
| <8 weeks | 3 | 0.04 (-0.21, 0.28) | 0.778 | 1.81 | 0.405 | 0 |
| >=8 weeks | 4 | -0.13 (-0.73, 0.47) | 0.676 | 1.48 | 0.686 | 0 |
| Dosage of hesperidin | ||||||
| <=500 mg/d | 3 | -0.11 (-0.70, 0.48) | 0.717 | 1.03 | 0.596 | 0 |
| >500 mg/d | 4 | 0.03 (-0.21, 0.28) | 0.792 | 2.31 | 0.510 | 0 |
| Baseline health status | ||||||
| Cardio-metabolic disorders | 5 | -0.25 (-0.74, 0.25) | 0.325 | 1.88 | 0.758 | 0 |
| Healthy | 2 | 0.08 (-0.17, 0.34) | 0.532 | 0.30 | 0.582 | 0 |
| Overall | 7 | 0.01 (-0.22, 0.24) | 0.918 | 3.54 | 0.739 | 0 |
| Body mass index (kg/m2) | ||||||
| Duration of intervention | ||||||
| <8 weeks | 4 | 0.04 (-0.03, 0.12) | 0.270 | 0.32 | 0.956 | 0 |
| >=8 weeks | 4 | -0.66 (-1.55, 0.23) | 0.148 | 6.56 | 0.087 | 54.2 |
| Dosage of hesperidin | ||||||
| <=500 mg/d | 4 | -0.01 (-0.18, 0.16) | 0.874 | 0.43 | 0.934 | 0 |
| >500 mg/d | 4 | -0.36 (-0.97, 0.25) | 0.252 | 8.85 | 0.031 | 66.1 |
| Baseline health status | ||||||
| Cardio-metabolic disorders | 6 | -0.16 (-0.55, 0.22) | 0.403 | 8.26 | 0.142 | 39.5 |
| Healthy | 2 | 0.04 (-0.04, 0.12) | 0.306 | 0.70 | 0.404 | 0 |
| Overall | 8 | -0.02 (-0.16, 0.13) | 0.831 | 9.58 | 0.214 | 26.9 |
| Waist circumference (cm) | ||||||
| Duration of intervention | ||||||
| <8 weeks | 2 | 0.40 (-0.14, 0.94) | 0.145 | 0.05 | 0.816 | 0 |
| >=8 weeks | 3 | -1.43 (-3.00, 0.14) | 0.074 | 3.51 | 0.173 | 43 |
| Dosage of hesperidin | ||||||
| <=500 mg/d | 2 | 0.15 (-0.64, 0.95) | 0.706 | 1.65 | 0.199 | 39.3 |
| >500 mg/d | 3 | -1.38 (-3.38, 0.63) | 0.178 | 4.53 | 0.104 | 55.9 |
| Baseline health status | ||||||
| Cardio-metabolic disorders | 4 | -0.67 (-2.15, 0.81) | 0.375 | 8.87 | 0.031 | 66.2 |
| Healthy | 1 | -0.46 (-1.68, 0.76) | 0.460 | 0.00 | - | - |
| Overall | 5 | -0.48 (-1.52, 0.55) | 0.362 | 9.76 | 0.045 | 59 |
| WMD: weighted wean difference | ||||||
Discussion
This meta-analysis quantifying evidence from RCTs found that intake of hesperidin had no statistically significant effects on the mean change differences in anthropometric indices compared to control groups. The results showed no different effects of hesperidin supplementation caused by the dosage and duration of treatment and the baseline health status of the participants. The findings were also robust in the sensitivity analyses.
Flavonoids are a widespread group of plant phenolic compounds which are commonly found in fruits and vegetables (Barreca et al., 2021). Although there is some evidence that flavonoids can be effective in weight loss, such favorable effects of hesperidin were not observed as a group of citrus flavonoids from the flavanones subclass. A meta-analysis by Akhlaghi et al. assessed the effects of flavonoid subclasses including flavonols, anthocyanins, flavanones, and proanthocyanidins on obesity-related anthropometric measures and found an overall significant reducing effect of total flavonoids on BMI and WC. This review suggested that among the flavonoid subgroups, only flavanols had a significant reducing effect on these markers and there was no effect for other flavonoid subclasses. However, no significant effect of total flavonoids and their subclasses was observed on body fat percentage (Akhlaghi et al., 2018).
Epidemiological evidence has also shown the role of flavonoids in weight maintenance. Three prospective cohort studies after assessing dietary intake of specific flavonoids reported that higher intake of most flavonoid subclasses was associated with less weight gain such that anthocyanins, flavonoid polymers, and flavonols had the greatest magnitude of association (Bertoia et al., 2016). On the other hand, there have been several recent systematic reviews and meta-analyses of clinical trials to summarize the efficacy of some of the individual flavonoids including resveratrol, curcumin, and quercetin in weight loss. These reviews reported that resveratrol (Mousavi et al., 2019) and curcumin (Akbari et al., 2019) led to a significant reduction in body weight, BMI, and WC; however, quercetin supplementation was not associated with significant changes in anthropometric measures (Huang et al., 2019). In the present review, hesperidin supplementation was not effective for changing anthropometric measurements. Therefore, it seems that the possible underlying mechanisms explaining the roles of several flavonoids in weight loss, such as reducing energy intake and fat absorption, increasing energy expenditure, and inhibiting adipogenesis and lipogenesis (Al Shukor et al., 2016) could not be generalized to all types of flavonoids.
Although in the present study, there is no evidence associated with the anti-obesity effects of hesperidin, it should be mentioned that the majority of the studies included in this review did not report anthropometric indices as the primary outcome measures, and therefore the measurements might not be sufficiently accurate. Only one of the studies by Ohara et al. directly assessed the anti-obesity effects of glucosyl hesperidin, a water-soluble derivative of hesperidin, with or without caffeine in moderately obese subjects. They showed that a concomitant intake of glucosyl hesperidin and caffeine reduced body weight, BMI, and abdominal fat; however, intake of glucosyl hesperidin alone showed no significant anti-obesity effect compared to the placebo group (Ohara et al., 2016). This is one of the limitations of this study and further investigations are thus required to directly assess the exact association between intake of hesperidin alone or in combination with other phytochemicals and changes in anthropometric measures as the primary outcomes. Also, the included studies have targeted a wide variety of populations including healthy adults and subjects with comorbidities such as obesity, hypercholesterolemia, metabolic syndrome, diabetes, myocardial infarction, and non-alcoholic fatty liver disease which made it difficult to determine the population that would most benefit from hesperidin. The bioavailability of hesperidin has not been also considered and evaluated in the included studies; therefore it is important to pay attention to this issue in future investigations to specify the precise concentrations of hesperidin available in the blood after ingestion and help to identify the ideal dosage of supplementation for maximum effectiveness. On the other hand, included RCTs were judged as being at unclear to high overall risk of bias and recruited a modest number of participants which creates the need for caution in the interpretation of results. Despite the limitations, a number of strengths can also be found in the present systematic review and meta‐analysis as follows: (i) design of search strategy to find all relevant published studies that reported anthropometric indices as initial or secondary outcomes, (ii) including only RCTs to minimize the potential biases, (iii) doing subgroups analysis and meta-regression, and (iv) lack of between-study heterogeneity and sensitivity of the pooled effects suggesting the robustness of findings.
Conclusion
The results of this systematic review and meta-analysis of available literature did not provide evidence for the beneficial effect of hesperidin as a citrus flavonoid in weight management. The current evidence suggests that daily hesperidin supplementation is not recommended as a potential therapeutic strategy for weight loss. However, due to the limitations of the included studies, future studies especially on overweight and obese individuals should be conducted to further understand the anti-obesity activity of hesperidin.
Acknowledgments
We thank Food Health Research Center, Hormozgan University of Medical Sciences, Bandar Abbas, Iran for funding this project.
Conflict of interest
The authors declare that they have no conflict of interest.
Author’s contributions
The authors’ contributions were as follows: all authors contributed in conceive and design the research; Ramezani-Jolfaie N and Mohammadi M conducted systematic research and study selection; Ramezani-Jolfaie N and Mohammadi M extracted data; Mohammadi M analyzed data; Ramezani-Jolfaie N and Lorzadeh E contributed in drafting of the manuscript; and all authors read and approved the final version for submission.
References
Akbari M, et al. 2019. The Effects of Curcumin on Weight Loss Among Patients With Metabolic Syndrome and Related Disorders: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Frontiers in pharmacology. 10: 649.
Akhlaghi M, Ghobadi S, Mohammad Hosseini M, Gholami Z & Mohammadian F 2018. Flavanols are potential anti-obesity agents, a systematic review and meta-analysis of controlled clinical trials. Nutrition, metabolism and cardiovascular diseases. 28 (7): 675-690.
Al Shukor N, Raes K, Smagghe G & Van Camp J 2016. Flavonoids: evidence for inhibitory effects against obesity and their possible mechanisms of action. Flavonoids and antioxidants. 40: 496-514.
Amiot MJ, Riva C & Vinet A 2016. Effects of dietary polyphenols on metabolic syndrome features in humans: a systematic review. Obesity reviews : an official journal of the International Association for the Study of Obesity. 17 (7): 573-586.
Barreca D, et al. 2021. Food flavonols: Nutraceuticals with complex health benefits and functionalities. Trends in food science & technology. 117: 194-204.
Barth SW, et al. 2012. Moderate effects of apple juice consumption on obesity-related markers in obese men: impact of diet-gene interaction on body fat content. European journal of nutrition. 51 (7): 841-850.
Bell ZW, Canale RE & Bloomer RJ 2011. A dual investigation of the effect of dietary supplementation with licorice flavonoid oil on anthropometric and biochemical markers of health and adiposity. Lipids in health and disease. 10: 29.
Bertoia ML, et al. 2016. Dietary flavonoid intake and weight maintenance: three prospective cohorts of 124,086 US men and women followed for up to 24 years. BMJ (Clinical research ed.). 352: i17.
Bonfrate L, Wang DQ, Garruti G & Portincasa P 2014. Obesity and the risk and prognosis of gallstone disease and pancreatitis. Best practice & research. Clinical gastroenterology. 28 (4): 623-635.
Briffa JF, McAinch AJ, Poronnik P & Hryciw DH 2013. Adipokines as a link between obesity and chronic kidney disease. American journal of physiology-renal physiology. 305 (12): F1629-F1636.
Butryn ML, Webb V & Wadden TA 2011. Behavioral treatment of obesity. Psychiatr Clin North Am. 34 (4): 841-859.
Cheraghpour M, et al. 2019. Hesperidin improves hepatic steatosis, hepatic enzymes, and metabolic and inflammatory parameters in patients with nonalcoholic fatty liver disease: A randomized, placebo‐controlled, double‐blind clinical trial. Phytotherapy research : PTR. 33 (8): 2118-2125.
Dallas C, et al. 2014. Clinical study to assess the efficacy and safety of a citrus polyphenolic extract of red orange, grapefruit, and orange (Sinetrol-XPur) on weight management and metabolic parameters in healthy overweight individuals. Phytotherapy research : PTR. 28 (2): 212-218.
Demonty I, et al. 2010. The citrus flavonoids hesperidin and naringin do not affect serum cholesterol in moderately hypercholesterolemic men and women. The Journal of nutrition. 140 (9): 1615-1620.
Derosa G & Maffioli P 2012. Anti-obesity drugs: a review about their effects and their safety. Expert opinion on drug safety. 11 (3): 459-471.
Donohoe CL, Lysaght J, O'Sullivan J & Reynolds JV 2017. Emerging concepts linking obesity with the hallmarks of cancer. Trends in endocrinology & metabolism. 28 (1): 46-62.
Egger M, Davey-Smith G & Altman D 2008. Systematic reviews in health care: meta-analysis in context. John Wiley & Sons.
Eghtesadi S, et al. 2016. Effects of hesperidin supplementation on glycemic control, lipid profile and inflammatory factors in patients with type 2 diabetes: a randomized, double-blind and placebo-controlled clinical trial. In Endocrine Abstracts. BioScientifica.
Genser L, Casella Mariolo JR, Castagneto-Gissey L, Panagiotopoulos S & Rubino F 2016. Obesity, Type 2 Diabetes, and the Metabolic Syndrome: Pathophysiologic Relationships and Guidelines for Surgical Intervention. The Surgical clinics of North America. 96 (4): 681-701.
Haidari F, et al. 2015. Hesperidin supplementation modulates inflammatory responses following myocardial infarction. Journal of the American college of nutrition. 34 (3): 205-211.
Harper JW & Zisman TL 2016. Interaction of obesity and inflammatory bowel disease. World journal of gastroenterology. 22 (35): 7868-7881.
Higgins JP & Green S 2011. Cochrane handbook for systematic reviews of interventions. John Wiley & Sons.
Homayouni F, Haidari F, Hedayati M, Zakerkish M & Ahmadi K 2017. Hesperidin Supplementation Alleviates Oxidative DNA Damage and Lipid Peroxidation in Type 2 Diabetes: A Randomized Double-Blind Placebo-Controlled Clinical Trial. Phytotherapy research : PTR. 31 (10): 1539-1545.
Homayouni F, Haidari F, Hedayati M, Zakerkish M & Ahmadi K 2018. Blood pressure lowering and anti-inflammatory effects of hesperidin in type 2 diabetes; a randomized double-blind controlled clinical trial. Phytotherapy research : PTR. 32 (6): 1073-1079.
Huang H, Liao D, Dong Y & Pu R 2019. Clinical effectiveness of quercetin supplementation in the management of weight loss: a pooled analysis of randomized controlled trials. Diabetes, metabolic syndrome and obesity. 12: 553-563.
Huisman S, Maes S, De Gucht VJ, Chatrou M & Haak HR 2010. Low goal ownership predicts drop-out from a weight intervention study in overweight patients with type 2 diabetes. Int J Behav Med. 17 (3): 176-181.
Janssens PL, Hursel R & Westerterp-Plantenga MS 2015. Long-term green tea extract supplementation does not affect fat absorption, resting energy expenditure, and body composition in adults. The Journal of nutrition. 145 (5): 864-870.
Kean RJ, et al. 2015. Chronic consumption of flavanone-rich orange juice is associated with cognitive benefits: an 8-wk, randomized, double-blind, placebo-controlled trial in healthy older adults. American journal of clinical nutrition. 101 (3): 506-514.
Khan A, Kim A, Sanossian C & Francois F 2016. Impact of obesity treatment on gastroesophageal reflux disease. World Journal of Gastroenterology. 22 (4): 1627.
Lamport DJ, et al. 2016. The effects of flavanone-rich citrus juice on cognitive function and cerebral blood flow: an acute, randomised, placebo-controlled cross-over trial in healthy, young adults. British journal of nutrition. 116 (12): 2160-2168.
Lehnert T, Sonntag D, Konnopka A, Riedel-Heller S & Konig HH 2013. Economic costs of overweight and obesity. Best practice & research. Clinical endocrinology & metabolism. 27 (2): 105-115.
Li L, et al. 2016. Obesity is an independent risk factor for non-alcoholic fatty liver disease: evidence from a meta-analysis of 21 cohort studies. Obesity reviews : an official journal of the International Association for the Study of Obesity. 17 (6): 510-519.
Lorzadeh E, Ramezani-Jolfaie N, Mohammadi M, Khoshbakht Y & Salehi-Abargouei A 2019. The effect of hesperidin supplementation on inflammatory markers in human adults: A systematic review and meta-analysis of randomized controlled clinical trials. Chemico-biological interactions. 307 (2019): 8-15.
Mandviwala T, Khalid U & Deswal A 2016. Obesity and cardiovascular disease: a risk factor or a risk marker? Current atherosclerosis reports. 18 (5): 21.
Martin-Jiménez CA, Gaitán-Vaca DM, Echeverria V, González J & Barreto GE 2017. Relationship between obesity, Alzheimer’s disease, and Parkinson’s disease: an astrocentric view. Molecular neurobiology. 54 (9): 7096-7115.
Martínez-Noguera FJ, Marín-Pagán C, Carlos-Vivas J & Alcaraz PE 2020. Effects of 8 Weeks of 2S-Hesperidin Supplementation on Performance in Amateur Cyclists. Nutrients. 12 (12): 3911.
Milenkovic D, Deval C, Dubray C, Mazur A & Morand C 2011. Hesperidin displays relevant role in the nutrigenomic effect of orange juice on blood leukocytes in human volunteers: a randomized controlled cross-over study. PloS one. 6 (11): e26669.
Miwa Y, et al. 2004. Effects of glucosyl hesperidin on serum lipids in hyperlipidemic subjects: preferential reduction in elevated serum triglyceride level. Journal of nutritional science and vitaminology. 50 (3): 211-218.
Mohammadi M, Ramezani-Jolfaie N, Lorzadeh E, Khoshbakht Y & Salehi-Abargouei A 2019. Hesperidin, a major flavonoid in orange juice, might not affect lipid profile and blood pressure: A systematic review and meta‐analysis of randomized controlled clinical trials. Phytotherapy research : PTR. 33 (3): 534-545.
Most J, Goossens GH, Jocken JW & Blaak EE 2014. Short-term supplementation with a specific combination of dietary polyphenols increases energy expenditure and alters substrate metabolism in overweight subjects. International journal of obesity (2005). 38 (5): 698-706.
Mousavi SM, et al. 2019. Resveratrol supplementation significantly influences obesity measures: a systematic review and dose-response meta-analysis of randomized controlled trials. Obesity reviews : an official journal of the International Association for the Study of Obesity. 20 (3): 487-498.
Mousavi SM, et al. 2018. Effect of Nigella sativa supplementation on obesity indices: A systematic review and meta-analysis of randomized controlled trials. Complementary therapies in medicine. 38: 48-57.
Mulvihill EE, Burke AC & Huff MW 2016. Citrus Flavonoids as Regulators of Lipoprotein Metabolism and Atherosclerosis. Annual review of nutrition. 36: 275-299.
Ng M, et al. 2014. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: a systematic analysis for the Global Burden of Disease Study 2013. lancet. 384 (9945): 766-781.
Ohara T, Muroyama K, Yamamoto Y & Murosaki S 2016. Oral intake of a combination of glucosyl hesperidin and caffeine elicits an anti-obesity effect in healthy, moderately obese subjects: a randomized double-blind placebo-controlled trial. Nutrition journal. 15 (1): 1-11.
Onakpoya I, Terry R & Ernst E 2011. The use of green coffee extract as a weight loss supplement: a systematic review and meta-analysis of randomised clinical trials. Gastroenterol Res Pract. 2011: 382852.
Orio F, et al. 2016. Obesity, type 2 diabetes mellitus and cardiovascular disease risk: an uptodate in the management of polycystic ovary syndrome. European journal of obstetrics & gynecology and reproductive biology. 207: 214-219.
Rangel-Huerta OD, et al. 2015. Normal or high polyphenol concentration in orange juice affects antioxidant activity, blood pressure, and body weight in obese or overweight adults. The Journal of nutrition. 145 (8): 1808-1816.
Ribeiro C, Dourado G & Cesar T 2017. Orange juice allied to a reduced-calorie diet results in weight loss and ameliorates obesity-related biomarkers: A randomized controlled trial. Nutrition. 38: 13-19.
Rizza S, et al. 2011. Citrus polyphenol hesperidin stimulates production of nitric oxide in endothelial cells while improving endothelial function and reducing inflammatory markers in patients with metabolic syndrome. Journal of clinical endocrinology & metabolism. 96 (5): E782-E792.
Roowi S, Mullen W, Edwards CA & Crozier A 2009. Yoghurt impacts on the excretion of phenolic acids derived from colonic breakdown of orange juice flavanones in humans. Molecular nutrition & food research. 53 (S1): S68-S75.
Salden BN, et al. 2016. Randomized clinical trial on the efficacy of hesperidin 2S on validated cardiovascular biomarkers in healthy overweight individuals. American journal of clinical nutrition. 104 (6): 1523-1533.
Schär MY, et al. 2015. Orange juice–derived flavanone and phenolic metabolites do not acutely affect cardiovascular risk biomarkers: a randomized, placebo-controlled, crossover trial in men at moderate risk of cardiovascular disease. American journal of clinical nutrition. 101 (5): 931-938.
Shams-Rad S, et al. 2020. Hesperidin supplementation has no effect on blood glucose control: A systematic review and meta-analysis of randomized controlled clinical trials. British journal of clinical pharmacology 86 (1): 13-22.
Shamseer L, et al. 2015. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: elaboration and explanation. BMJ (Clinical research ed.). 350: g7647.
Simpson EJ, Mendis B & Macdonald IA 2016. Orange juice consumption and its effect on blood lipid profile and indices of the metabolic syndrome; a randomised, controlled trial in an at-risk population. Food & function. 7 (4): 1884-1891.
Soeliman FA & Azadbakht L 2014. Weight loss maintenance: A review on dietary related strategies. Journal of research in medical sciences : the official journal of Isfahan University of Medical Sciences. 19 (3): 268-275.
Stoner L & Cornwall J 2014. Did the American Medical Association make the correct decision classifying obesity as a disease? Australasian medical journal. 7 (11): 462-464.
Thomas DM, et al. 2014. Dynamic model predicting overweight, obesity, and extreme obesity prevalence trends. Obesity. 22 (2): 590-597.
Tuomilehto J, et al. 2001. Prevention of type 2 diabetes mellitus by changes in lifestyle among subjects with impaired glucose tolerance. New England journal of medicine. 344 (18): 1343-1350.
Valls RM, et al. 2021a. Hesperidin in orange juice improves human endothelial function in subjects with elevated blood pressure and stage 1 hypertension: a randomized, controlled trial (Citrus study). Journal of functional foods. 85: 104646.
Valls RM, et al. 2021b. Effects of hesperidin in orange juice on blood and pulse pressures in mildly hypertensive individuals: a randomized controlled trial (Citrus study). European journal of nutrition. 60 (3): 1277-1288.
World Health Organization October 2017. Obesity and overweight fact sheet. www.who.int/en/news-room/fact-sheets/detail/obesity-and-overweight.
Yari Z, et al. 2021a. The efficacy of flaxseed and hesperidin on non-alcoholic fatty liver disease: an open-labeled randomized controlled trial. European journal of clinical nutrition. 75 (1): 99-111.
Yari Z, Cheraghpour M & Hekmatdoost A 2021b. Flaxseed and/or hesperidin supplementation in metabolic syndrome: An open-labeled randomized controlled trial. European journal of nutrition. 60 (1): 287-298.
Yari Z, et al. 2019. The effect of hesperidin supplementation on metabolic profiles in patients with metabolic syndrome: a randomized, double-blind, placebo-controlled clinical trial. European journal of nutrition.
Yari Z, et al. 2021c. Combination therapy of flaxseed and hesperidin enhances the effectiveness of lifestyle modification in cardiovascular risk control in prediabetes: a randomized controlled trial. Diabetology & metabolic syndrome. 13 (1): 1-11.
Yoshitomi R, et al. 2021. The combined effect of green tea and alpha-glucosyl hesperidin in preventing obesity: a randomized placebo-controlled clinical trial. Scientific reports. 11 (1): 19067.
Zuckoff A 2012. "Why won't my patients do what's good for them?" Motivational interviewing and treatment adherence. Surgery for obesity and related diseases. 8 (5): 514-521.
This meta-analysis quantifying evidence from RCTs found that intake of hesperidin had no statistically significant effects on the mean change differences in anthropometric indices compared to control groups. The results showed no different effects of hesperidin supplementation caused by the dosage and duration of treatment and the baseline health status of the participants. The findings were also robust in the sensitivity analyses.
Flavonoids are a widespread group of plant phenolic compounds which are commonly found in fruits and vegetables (Barreca et al., 2021). Although there is some evidence that flavonoids can be effective in weight loss, such favorable effects of hesperidin were not observed as a group of citrus flavonoids from the flavanones subclass. A meta-analysis by Akhlaghi et al. assessed the effects of flavonoid subclasses including flavonols, anthocyanins, flavanones, and proanthocyanidins on obesity-related anthropometric measures and found an overall significant reducing effect of total flavonoids on BMI and WC. This review suggested that among the flavonoid subgroups, only flavanols had a significant reducing effect on these markers and there was no effect for other flavonoid subclasses. However, no significant effect of total flavonoids and their subclasses was observed on body fat percentage (Akhlaghi et al., 2018).
Epidemiological evidence has also shown the role of flavonoids in weight maintenance. Three prospective cohort studies after assessing dietary intake of specific flavonoids reported that higher intake of most flavonoid subclasses was associated with less weight gain such that anthocyanins, flavonoid polymers, and flavonols had the greatest magnitude of association (Bertoia et al., 2016). On the other hand, there have been several recent systematic reviews and meta-analyses of clinical trials to summarize the efficacy of some of the individual flavonoids including resveratrol, curcumin, and quercetin in weight loss. These reviews reported that resveratrol (Mousavi et al., 2019) and curcumin (Akbari et al., 2019) led to a significant reduction in body weight, BMI, and WC; however, quercetin supplementation was not associated with significant changes in anthropometric measures (Huang et al., 2019). In the present review, hesperidin supplementation was not effective for changing anthropometric measurements. Therefore, it seems that the possible underlying mechanisms explaining the roles of several flavonoids in weight loss, such as reducing energy intake and fat absorption, increasing energy expenditure, and inhibiting adipogenesis and lipogenesis (Al Shukor et al., 2016) could not be generalized to all types of flavonoids.
Although in the present study, there is no evidence associated with the anti-obesity effects of hesperidin, it should be mentioned that the majority of the studies included in this review did not report anthropometric indices as the primary outcome measures, and therefore the measurements might not be sufficiently accurate. Only one of the studies by Ohara et al. directly assessed the anti-obesity effects of glucosyl hesperidin, a water-soluble derivative of hesperidin, with or without caffeine in moderately obese subjects. They showed that a concomitant intake of glucosyl hesperidin and caffeine reduced body weight, BMI, and abdominal fat; however, intake of glucosyl hesperidin alone showed no significant anti-obesity effect compared to the placebo group (Ohara et al., 2016). This is one of the limitations of this study and further investigations are thus required to directly assess the exact association between intake of hesperidin alone or in combination with other phytochemicals and changes in anthropometric measures as the primary outcomes. Also, the included studies have targeted a wide variety of populations including healthy adults and subjects with comorbidities such as obesity, hypercholesterolemia, metabolic syndrome, diabetes, myocardial infarction, and non-alcoholic fatty liver disease which made it difficult to determine the population that would most benefit from hesperidin. The bioavailability of hesperidin has not been also considered and evaluated in the included studies; therefore it is important to pay attention to this issue in future investigations to specify the precise concentrations of hesperidin available in the blood after ingestion and help to identify the ideal dosage of supplementation for maximum effectiveness. On the other hand, included RCTs were judged as being at unclear to high overall risk of bias and recruited a modest number of participants which creates the need for caution in the interpretation of results. Despite the limitations, a number of strengths can also be found in the present systematic review and meta‐analysis as follows: (i) design of search strategy to find all relevant published studies that reported anthropometric indices as initial or secondary outcomes, (ii) including only RCTs to minimize the potential biases, (iii) doing subgroups analysis and meta-regression, and (iv) lack of between-study heterogeneity and sensitivity of the pooled effects suggesting the robustness of findings.
Conclusion
The results of this systematic review and meta-analysis of available literature did not provide evidence for the beneficial effect of hesperidin as a citrus flavonoid in weight management. The current evidence suggests that daily hesperidin supplementation is not recommended as a potential therapeutic strategy for weight loss. However, due to the limitations of the included studies, future studies especially on overweight and obese individuals should be conducted to further understand the anti-obesity activity of hesperidin.
Acknowledgments
We thank Food Health Research Center, Hormozgan University of Medical Sciences, Bandar Abbas, Iran for funding this project.
Conflict of interest
The authors declare that they have no conflict of interest.
Author’s contributions
The authors’ contributions were as follows: all authors contributed in conceive and design the research; Ramezani-Jolfaie N and Mohammadi M conducted systematic research and study selection; Ramezani-Jolfaie N and Mohammadi M extracted data; Mohammadi M analyzed data; Ramezani-Jolfaie N and Lorzadeh E contributed in drafting of the manuscript; and all authors read and approved the final version for submission.
References
Akbari M, et al. 2019. The Effects of Curcumin on Weight Loss Among Patients With Metabolic Syndrome and Related Disorders: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Frontiers in pharmacology. 10: 649.
Akhlaghi M, Ghobadi S, Mohammad Hosseini M, Gholami Z & Mohammadian F 2018. Flavanols are potential anti-obesity agents, a systematic review and meta-analysis of controlled clinical trials. Nutrition, metabolism and cardiovascular diseases. 28 (7): 675-690.
Al Shukor N, Raes K, Smagghe G & Van Camp J 2016. Flavonoids: evidence for inhibitory effects against obesity and their possible mechanisms of action. Flavonoids and antioxidants. 40: 496-514.
Amiot MJ, Riva C & Vinet A 2016. Effects of dietary polyphenols on metabolic syndrome features in humans: a systematic review. Obesity reviews : an official journal of the International Association for the Study of Obesity. 17 (7): 573-586.
Barreca D, et al. 2021. Food flavonols: Nutraceuticals with complex health benefits and functionalities. Trends in food science & technology. 117: 194-204.
Barth SW, et al. 2012. Moderate effects of apple juice consumption on obesity-related markers in obese men: impact of diet-gene interaction on body fat content. European journal of nutrition. 51 (7): 841-850.
Bell ZW, Canale RE & Bloomer RJ 2011. A dual investigation of the effect of dietary supplementation with licorice flavonoid oil on anthropometric and biochemical markers of health and adiposity. Lipids in health and disease. 10: 29.
Bertoia ML, et al. 2016. Dietary flavonoid intake and weight maintenance: three prospective cohorts of 124,086 US men and women followed for up to 24 years. BMJ (Clinical research ed.). 352: i17.
Bonfrate L, Wang DQ, Garruti G & Portincasa P 2014. Obesity and the risk and prognosis of gallstone disease and pancreatitis. Best practice & research. Clinical gastroenterology. 28 (4): 623-635.
Briffa JF, McAinch AJ, Poronnik P & Hryciw DH 2013. Adipokines as a link between obesity and chronic kidney disease. American journal of physiology-renal physiology. 305 (12): F1629-F1636.
Butryn ML, Webb V & Wadden TA 2011. Behavioral treatment of obesity. Psychiatr Clin North Am. 34 (4): 841-859.
Cheraghpour M, et al. 2019. Hesperidin improves hepatic steatosis, hepatic enzymes, and metabolic and inflammatory parameters in patients with nonalcoholic fatty liver disease: A randomized, placebo‐controlled, double‐blind clinical trial. Phytotherapy research : PTR. 33 (8): 2118-2125.
Dallas C, et al. 2014. Clinical study to assess the efficacy and safety of a citrus polyphenolic extract of red orange, grapefruit, and orange (Sinetrol-XPur) on weight management and metabolic parameters in healthy overweight individuals. Phytotherapy research : PTR. 28 (2): 212-218.
Demonty I, et al. 2010. The citrus flavonoids hesperidin and naringin do not affect serum cholesterol in moderately hypercholesterolemic men and women. The Journal of nutrition. 140 (9): 1615-1620.
Derosa G & Maffioli P 2012. Anti-obesity drugs: a review about their effects and their safety. Expert opinion on drug safety. 11 (3): 459-471.
Donohoe CL, Lysaght J, O'Sullivan J & Reynolds JV 2017. Emerging concepts linking obesity with the hallmarks of cancer. Trends in endocrinology & metabolism. 28 (1): 46-62.
Egger M, Davey-Smith G & Altman D 2008. Systematic reviews in health care: meta-analysis in context. John Wiley & Sons.
Eghtesadi S, et al. 2016. Effects of hesperidin supplementation on glycemic control, lipid profile and inflammatory factors in patients with type 2 diabetes: a randomized, double-blind and placebo-controlled clinical trial. In Endocrine Abstracts. BioScientifica.
Genser L, Casella Mariolo JR, Castagneto-Gissey L, Panagiotopoulos S & Rubino F 2016. Obesity, Type 2 Diabetes, and the Metabolic Syndrome: Pathophysiologic Relationships and Guidelines for Surgical Intervention. The Surgical clinics of North America. 96 (4): 681-701.
Haidari F, et al. 2015. Hesperidin supplementation modulates inflammatory responses following myocardial infarction. Journal of the American college of nutrition. 34 (3): 205-211.
Harper JW & Zisman TL 2016. Interaction of obesity and inflammatory bowel disease. World journal of gastroenterology. 22 (35): 7868-7881.
Higgins JP & Green S 2011. Cochrane handbook for systematic reviews of interventions. John Wiley & Sons.
Homayouni F, Haidari F, Hedayati M, Zakerkish M & Ahmadi K 2017. Hesperidin Supplementation Alleviates Oxidative DNA Damage and Lipid Peroxidation in Type 2 Diabetes: A Randomized Double-Blind Placebo-Controlled Clinical Trial. Phytotherapy research : PTR. 31 (10): 1539-1545.
Homayouni F, Haidari F, Hedayati M, Zakerkish M & Ahmadi K 2018. Blood pressure lowering and anti-inflammatory effects of hesperidin in type 2 diabetes; a randomized double-blind controlled clinical trial. Phytotherapy research : PTR. 32 (6): 1073-1079.
Huang H, Liao D, Dong Y & Pu R 2019. Clinical effectiveness of quercetin supplementation in the management of weight loss: a pooled analysis of randomized controlled trials. Diabetes, metabolic syndrome and obesity. 12: 553-563.
Huisman S, Maes S, De Gucht VJ, Chatrou M & Haak HR 2010. Low goal ownership predicts drop-out from a weight intervention study in overweight patients with type 2 diabetes. Int J Behav Med. 17 (3): 176-181.
Janssens PL, Hursel R & Westerterp-Plantenga MS 2015. Long-term green tea extract supplementation does not affect fat absorption, resting energy expenditure, and body composition in adults. The Journal of nutrition. 145 (5): 864-870.
Kean RJ, et al. 2015. Chronic consumption of flavanone-rich orange juice is associated with cognitive benefits: an 8-wk, randomized, double-blind, placebo-controlled trial in healthy older adults. American journal of clinical nutrition. 101 (3): 506-514.
Khan A, Kim A, Sanossian C & Francois F 2016. Impact of obesity treatment on gastroesophageal reflux disease. World Journal of Gastroenterology. 22 (4): 1627.
Lamport DJ, et al. 2016. The effects of flavanone-rich citrus juice on cognitive function and cerebral blood flow: an acute, randomised, placebo-controlled cross-over trial in healthy, young adults. British journal of nutrition. 116 (12): 2160-2168.
Lehnert T, Sonntag D, Konnopka A, Riedel-Heller S & Konig HH 2013. Economic costs of overweight and obesity. Best practice & research. Clinical endocrinology & metabolism. 27 (2): 105-115.
Li L, et al. 2016. Obesity is an independent risk factor for non-alcoholic fatty liver disease: evidence from a meta-analysis of 21 cohort studies. Obesity reviews : an official journal of the International Association for the Study of Obesity. 17 (6): 510-519.
Lorzadeh E, Ramezani-Jolfaie N, Mohammadi M, Khoshbakht Y & Salehi-Abargouei A 2019. The effect of hesperidin supplementation on inflammatory markers in human adults: A systematic review and meta-analysis of randomized controlled clinical trials. Chemico-biological interactions. 307 (2019): 8-15.
Mandviwala T, Khalid U & Deswal A 2016. Obesity and cardiovascular disease: a risk factor or a risk marker? Current atherosclerosis reports. 18 (5): 21.
Martin-Jiménez CA, Gaitán-Vaca DM, Echeverria V, González J & Barreto GE 2017. Relationship between obesity, Alzheimer’s disease, and Parkinson’s disease: an astrocentric view. Molecular neurobiology. 54 (9): 7096-7115.
Martínez-Noguera FJ, Marín-Pagán C, Carlos-Vivas J & Alcaraz PE 2020. Effects of 8 Weeks of 2S-Hesperidin Supplementation on Performance in Amateur Cyclists. Nutrients. 12 (12): 3911.
Milenkovic D, Deval C, Dubray C, Mazur A & Morand C 2011. Hesperidin displays relevant role in the nutrigenomic effect of orange juice on blood leukocytes in human volunteers: a randomized controlled cross-over study. PloS one. 6 (11): e26669.
Miwa Y, et al. 2004. Effects of glucosyl hesperidin on serum lipids in hyperlipidemic subjects: preferential reduction in elevated serum triglyceride level. Journal of nutritional science and vitaminology. 50 (3): 211-218.
Mohammadi M, Ramezani-Jolfaie N, Lorzadeh E, Khoshbakht Y & Salehi-Abargouei A 2019. Hesperidin, a major flavonoid in orange juice, might not affect lipid profile and blood pressure: A systematic review and meta‐analysis of randomized controlled clinical trials. Phytotherapy research : PTR. 33 (3): 534-545.
Most J, Goossens GH, Jocken JW & Blaak EE 2014. Short-term supplementation with a specific combination of dietary polyphenols increases energy expenditure and alters substrate metabolism in overweight subjects. International journal of obesity (2005). 38 (5): 698-706.
Mousavi SM, et al. 2019. Resveratrol supplementation significantly influences obesity measures: a systematic review and dose-response meta-analysis of randomized controlled trials. Obesity reviews : an official journal of the International Association for the Study of Obesity. 20 (3): 487-498.
Mousavi SM, et al. 2018. Effect of Nigella sativa supplementation on obesity indices: A systematic review and meta-analysis of randomized controlled trials. Complementary therapies in medicine. 38: 48-57.
Mulvihill EE, Burke AC & Huff MW 2016. Citrus Flavonoids as Regulators of Lipoprotein Metabolism and Atherosclerosis. Annual review of nutrition. 36: 275-299.
Ng M, et al. 2014. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: a systematic analysis for the Global Burden of Disease Study 2013. lancet. 384 (9945): 766-781.
Ohara T, Muroyama K, Yamamoto Y & Murosaki S 2016. Oral intake of a combination of glucosyl hesperidin and caffeine elicits an anti-obesity effect in healthy, moderately obese subjects: a randomized double-blind placebo-controlled trial. Nutrition journal. 15 (1): 1-11.
Onakpoya I, Terry R & Ernst E 2011. The use of green coffee extract as a weight loss supplement: a systematic review and meta-analysis of randomised clinical trials. Gastroenterol Res Pract. 2011: 382852.
Orio F, et al. 2016. Obesity, type 2 diabetes mellitus and cardiovascular disease risk: an uptodate in the management of polycystic ovary syndrome. European journal of obstetrics & gynecology and reproductive biology. 207: 214-219.
Rangel-Huerta OD, et al. 2015. Normal or high polyphenol concentration in orange juice affects antioxidant activity, blood pressure, and body weight in obese or overweight adults. The Journal of nutrition. 145 (8): 1808-1816.
Ribeiro C, Dourado G & Cesar T 2017. Orange juice allied to a reduced-calorie diet results in weight loss and ameliorates obesity-related biomarkers: A randomized controlled trial. Nutrition. 38: 13-19.
Rizza S, et al. 2011. Citrus polyphenol hesperidin stimulates production of nitric oxide in endothelial cells while improving endothelial function and reducing inflammatory markers in patients with metabolic syndrome. Journal of clinical endocrinology & metabolism. 96 (5): E782-E792.
Roowi S, Mullen W, Edwards CA & Crozier A 2009. Yoghurt impacts on the excretion of phenolic acids derived from colonic breakdown of orange juice flavanones in humans. Molecular nutrition & food research. 53 (S1): S68-S75.
Salden BN, et al. 2016. Randomized clinical trial on the efficacy of hesperidin 2S on validated cardiovascular biomarkers in healthy overweight individuals. American journal of clinical nutrition. 104 (6): 1523-1533.
Schär MY, et al. 2015. Orange juice–derived flavanone and phenolic metabolites do not acutely affect cardiovascular risk biomarkers: a randomized, placebo-controlled, crossover trial in men at moderate risk of cardiovascular disease. American journal of clinical nutrition. 101 (5): 931-938.
Shams-Rad S, et al. 2020. Hesperidin supplementation has no effect on blood glucose control: A systematic review and meta-analysis of randomized controlled clinical trials. British journal of clinical pharmacology 86 (1): 13-22.
Shamseer L, et al. 2015. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: elaboration and explanation. BMJ (Clinical research ed.). 350: g7647.
Simpson EJ, Mendis B & Macdonald IA 2016. Orange juice consumption and its effect on blood lipid profile and indices of the metabolic syndrome; a randomised, controlled trial in an at-risk population. Food & function. 7 (4): 1884-1891.
Soeliman FA & Azadbakht L 2014. Weight loss maintenance: A review on dietary related strategies. Journal of research in medical sciences : the official journal of Isfahan University of Medical Sciences. 19 (3): 268-275.
Stoner L & Cornwall J 2014. Did the American Medical Association make the correct decision classifying obesity as a disease? Australasian medical journal. 7 (11): 462-464.
Thomas DM, et al. 2014. Dynamic model predicting overweight, obesity, and extreme obesity prevalence trends. Obesity. 22 (2): 590-597.
Tuomilehto J, et al. 2001. Prevention of type 2 diabetes mellitus by changes in lifestyle among subjects with impaired glucose tolerance. New England journal of medicine. 344 (18): 1343-1350.
Valls RM, et al. 2021a. Hesperidin in orange juice improves human endothelial function in subjects with elevated blood pressure and stage 1 hypertension: a randomized, controlled trial (Citrus study). Journal of functional foods. 85: 104646.
Valls RM, et al. 2021b. Effects of hesperidin in orange juice on blood and pulse pressures in mildly hypertensive individuals: a randomized controlled trial (Citrus study). European journal of nutrition. 60 (3): 1277-1288.
World Health Organization October 2017. Obesity and overweight fact sheet. www.who.int/en/news-room/fact-sheets/detail/obesity-and-overweight.
Yari Z, et al. 2021a. The efficacy of flaxseed and hesperidin on non-alcoholic fatty liver disease: an open-labeled randomized controlled trial. European journal of clinical nutrition. 75 (1): 99-111.
Yari Z, Cheraghpour M & Hekmatdoost A 2021b. Flaxseed and/or hesperidin supplementation in metabolic syndrome: An open-labeled randomized controlled trial. European journal of nutrition. 60 (1): 287-298.
Yari Z, et al. 2019. The effect of hesperidin supplementation on metabolic profiles in patients with metabolic syndrome: a randomized, double-blind, placebo-controlled clinical trial. European journal of nutrition.
Yari Z, et al. 2021c. Combination therapy of flaxseed and hesperidin enhances the effectiveness of lifestyle modification in cardiovascular risk control in prediabetes: a randomized controlled trial. Diabetology & metabolic syndrome. 13 (1): 1-11.
Yoshitomi R, et al. 2021. The combined effect of green tea and alpha-glucosyl hesperidin in preventing obesity: a randomized placebo-controlled clinical trial. Scientific reports. 11 (1): 19067.
Zuckoff A 2012. "Why won't my patients do what's good for them?" Motivational interviewing and treatment adherence. Surgery for obesity and related diseases. 8 (5): 514-521.
Type of article: review article |
Subject:
public specific
Received: 2022/03/26 | Published: 2023/11/20 | ePublished: 2023/11/20
Received: 2022/03/26 | Published: 2023/11/20 | ePublished: 2023/11/20
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
