
Wed, Jul 29, 2026
[Archive]
Volume 7, Issue 4 (NOV 2022)
JNFS 2022, 7(4): 548-561 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Ahmadi Vasmehjani A, Yaghoubi F, Darabi Z, Abdollahi N, Sangsefidi Z S, Hosseinzadeh M. The effect of quercetin on stress The Effect of Quercetin on Stress Oxidative Markers: A Systematic Review and Meta-Analysis of Randomized Controlled Clinical Trialsers; A systematic review and meta-analysis of randomized controlled clinical trials. JNFS 2022; 7 (4) :548-561
URL: http://jnfs.ssu.ac.ir/article-1-416-en.html
URL: http://jnfs.ssu.ac.ir/article-1-416-en.html
Azam Ahmadi Vasmehjani 

 , Fatemeh Yaghoubi , Zahra Darabi , Nooshin Abdollahi , Zohreh Sadat Sangsefidi , Mahdieh Hosseinzadeh *
, Fatemeh Yaghoubi , Zahra Darabi , Nooshin Abdollahi , Zohreh Sadat Sangsefidi , Mahdieh Hosseinzadeh *
, Fatemeh Yaghoubi , Zahra Darabi , Nooshin Abdollahi , Zohreh Sadat Sangsefidi , Mahdieh Hosseinzadeh *
Department of Nutrition, School of Public Health, Shahid Sadoughi University of Medical Sciences, Yazd, Iran
Keywords: Quercetin, Oxidative stress, Malondialdehyde, Total antioxidant capacity, Ferric reducing ability of plasma
Full-Text [PDF 729 kb]
(1210 Downloads)
| Abstract (HTML) (5047 Views)
Characteristics of studies: The details of the 8 included studies are presented in Table 2. Studies were listed based on the following information: country, age(y), gender, sample size (intervention), RCT design, intervention name, quercetin dosage, name control, duration, outcome, and health status of participants. Studies were published from 2007 to 2020 and sample size ranged from 8 to 668 participants. Cross-over design was in two studies. The intervention duration in the trials was
.JPG)
.JPG)
.JPG)
.JPG)
.JPG)
.JPG)
Full-Text: (1757 Views)
The Effect of Quercetin on Stress Oxidative Markers: A Systematic Review and Meta-Analysis of Randomized Controlled Clinical Trials
Azam Ahmadi Vasmehjani; MSc 1,2, Fatemeh Yaghoubi; PhD 2,3 , Zahra Darabi; MSc 1,2,
Nooshin Abdollahi; MSc 1,2, Zohreh Sadat Sangsefidi; PhD 4 & Mahdieh Hosseinzadeh; PhD *1,2
1 Department of Nutrition, School of Public Health, Shahid Sadoughi University of Medical Sciences, Yazd, Iran;
2 Nutrition and Food Security Research Center, Shahid Sadoughi University of Medical Sciences, Yazd, Iran;
3 Department of Biochemistry, School of Medicine, Shahid Sadoughi University of Medical Sciences, Yazd, Iran; 4 Department of Nutrition, School of Public of Health, North Khorasan University of Medical Sciences, Bojnurd, Iran.
Azam Ahmadi Vasmehjani; MSc 1,2, Fatemeh Yaghoubi; PhD 2,3 , Zahra Darabi; MSc 1,2,
Nooshin Abdollahi; MSc 1,2, Zohreh Sadat Sangsefidi; PhD 4 & Mahdieh Hosseinzadeh; PhD *1,2
1 Department of Nutrition, School of Public Health, Shahid Sadoughi University of Medical Sciences, Yazd, Iran;
2 Nutrition and Food Security Research Center, Shahid Sadoughi University of Medical Sciences, Yazd, Iran;
3 Department of Biochemistry, School of Medicine, Shahid Sadoughi University of Medical Sciences, Yazd, Iran; 4 Department of Nutrition, School of Public of Health, North Khorasan University of Medical Sciences, Bojnurd, Iran.
| ARTICLE INFO | ABSTRACT | |
| SYSTEMATIC REVIEW and META-ANALYSIS | Background: Quercetin is one of the main flavonoids, overall distributed in plants. The antioxidant capacity of quercetin is several times vitamin E and glutathione. This systematic review and meta‐analysis of randomized controlled trials were performed to determine the effect of quercetin on oxidative stress (OS) markers. Methods: A literature search was conducted in PubMed, ISI Web of Science, Scopus, and Google Scholar to February of 2021. Meta-analysis was conducted on 8 eligible RCTs containing a total of 668 participants. The weighted mean difference (WMD) with 95% confidence intervals (CIs) was calculated for a pool effect size of Malondialdehyde (MDA), Total Antioxidant Capacity (TAC), and Ferric Reducing Ability of Plasma (FRAP). Subgroup analyses were performed based on intervention duration and dosage. The heterogeneity of studies was examined by Cochran's Q test and I-squared (I2) statistic. Results: Effect sizes from 668 participants based on the random effect model showed that quercetin supplementation had no significant effect on TAC and MDA compared to the control group. The analysis illustrated that quercetin supplementation significantly increased FRAP in adults (WMD = -0.159 mmol/l, 95% confidence interval (CI):-0.178, -0.141, P ≤ 0.001). Conclusions: The finding of the current study showed that quercetin supplementation had no significant effect on TAC levels, although it significantly increased FRAP levels in adults. Also, MDA level did not markedly change. It has needed to conduct clinical trials with more quality and bigger sample sizes to verify the positive impact of quercetin on stress oxidative marker. Keywords: Quercetin; Oxidative stress; Malondialdehyde; Total antioxidant capacity; Ferric reducing ability of plasma |
|
| Article history: Received: 27 May 2021 Revised: 30 Aug 2021 Accepted: 6 Sep 2021 |
||
| *Corresponding author: hoseinzade.mahdie@gmail.com Mahdieh Hosseinzadeh, Department of Nutrition, School of Public Health, Sahid Sadoughi University of Medical Sciences, Yazd, Iran. Postal code: 13145-158 Tel: +98 9385783858 |
Introduction
Oxidative stress (OS) is a potential injurious mechanism to human health. It plays a predominant role in the origination of reactive oxygen species (ROS) (van't Erve, 2018). ROS reacts with proteins, membrane lipids, and nucleic acids directly which causes disrupting cellular function. Finally OS can designate to pathological diseases, such as cancer, neurological disorders, atherosclerosis, hypertension, ischemia/perfusion, diabetes, acute respiratory distress syndrome, idiopathic pulmonary fibrosis, chronic obstructive pulmonary disease, and asthma (Birben et al., 2012, Sepidarkish et al., 2019, Sties et al., 2018, van't Erve, 2018). Any other way, cell defense systems have integrated antioxidant systems, which consist of enzymatic and non-enzymatic antioxidants. Enzymatic antioxidants include superoxide dismutase (SOD), catalase (CAT), and glutathione peroxidase (GPX) (Linke et al., 2005, Sties et al., 2018). OS occurs when the natural production of ROS cannot be balanced by the anti-oxidative capacity of tissues (Barja, 2013). Many studies have focused on strategies to reduce OS with the goal of bettering health. Diet modification or utilization of supplementation are used to change antioxidants levels (van't Erve, 2018). One of the must usually ways for scavenger of ROS is Quercetin. Antioxidant capacity of quercetin is several times that of endogenous antioxidants consisting of vitamin E and glutathione (Boots et al., 2011). It is one of the main flavonoids, overall distributed in (edible) plants (Egert et al., 2009). Onions, kale, unpeeled apples berries, citrus fruits, and tea (Camellia sinensis) are affluent sources of quercetin (Brüll et al., 2015). Some studies have shown that quercetin has manifested diversity of bioactive effects, such as antioxidant, anti-inflammatory, antimicrobial, antibacterial, and vasodilatory actions (Bazzucchi et al., 2019, Brüll et al., 2015, Egert et al., 2009). In addition it has been realized to exert anti-aging, antithrombotic, anti aggregatory, and vasodilatory effects (Riva et al., 2019). Some randomized controlled trials (RCTs) have examined the effects of quercetin on OS markers in diverse population, whereas the results are disagreed (Egert et al., 2008, Scholten and Sergeev, 2013).
To the best of the authors’ knowledge, there is no systematic review or meta‐ analysis study to assess the impact of quercetin administration on the OS markers in human. Thus, this meta‐analysis aims to summarize the present evidence of RCTs on the effects of quercetin supplementation on OS markers among diverse population.
To the best of the authors’ knowledge, there is no systematic review or meta‐ analysis study to assess the impact of quercetin administration on the OS markers in human. Thus, this meta‐analysis aims to summarize the present evidence of RCTs on the effects of quercetin supplementation on OS markers among diverse population.
Materials and Methods
Protocol and search strategy: The protocol of the current study was registered in the international prospective register of systematic reviews (PROSPERO) database (http://www.crd.york.ac.uk/PROSPERO), with registration code of CRD42020219056. This review was performed based on Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist (Liberati et al., 2009). Medical electronic databases, including Scopus, Web of Science and PubMed, and Google Scholar were searched up to 15th Februay 2021. Medical Subject Heading (MeSH) terms and non-MeSH terms were applied to the effect of quercetin on oxidative stress markers. The following keywords were used to search with consideration of the wide range of synonyms used in literature. "Quercetin", "OS", "Malondialdehyde", "Thiobarbituric Acid Reactive Substances", "oxidative mediators", "OS markers", "Superoxide Dismutase", "Glutathione Peroxidase", "Catalase", "Glutathione", "GSH", "Glutathione Reductase", "total antioxidant capacity", "TAC", "Oxygen Radical Absorbance Capacity", "ORAC", "total oxidant status", and "F2-Isoprostanes". The study also examined the citation lists of review articles, correlated publications, and selection studies references to find pertinent studies. The results from search in different databases were mixed, and duplicates were removed.
Inclusion criteria:
1. Randomized controlled trials parallel or cross-over either drug or placebo design
2. Studies that investigated the effects of quercetin supplementation on OS parameters
3. Studies that implement sufficient data on OS parameters at baseline and at the end of the intervention in both quercetin and placebo groups to identify the difference in mean values with 95% confidence intervals (CIs).
4. Participants aged ≥18 years
5. Presented the prescribed dosage
2. Studies that investigated the effects of quercetin supplementation on OS parameters
3. Studies that implement sufficient data on OS parameters at baseline and at the end of the intervention in both quercetin and placebo groups to identify the difference in mean values with 95% confidence intervals (CIs).
4. Participants aged ≥18 years
5. Presented the prescribed dosage
Exclusion criteria:
1. Experimental studies, in vitro studies, case reports, observational studies, review articles, letters to the editor, and editorials were excluded from this meta‐analysis.
2. Studies without control group also, in which other interventions were used along with
quercetin supplementation were excluded from this meta‐analysis.
2. Studies without control group also, in which other interventions were used along with
quercetin supplementation were excluded from this meta‐analysis.
Study selection: After removing duplicates, title and abstract screening was independently conducted by two reviewers (Ahmadi Vasmehjani A and Darabi Z), then relevant full texts were investigated and authors were contacted for those were unavailable and unclear.
Data extraction: The following data from each study was extracted: the author's name and the year of publication and country of origin; property of the participants (age, gender), duration of trial, RCT design, health status of participants; sample size (experimental group/controlled group); the duration of intervention; dosage of intervention; and the mean and standard deviation for major outcome. Data extraction was done by two investigators, independently (Ahmadi Vasmehjani A and Darabi Z) using a designed form according to the inclusion and exclusion criteria.
Risk of bias assessment: The quality assessment of selected RCTs was doing via the Cochrane Collaboration risk of bias tool based of random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete data, and selective reporting (Lorzadeh et al., 2019).
Data synthesis and analysis: The effects of quercetin supplementation on the changes of the following outcomes were calculated; MDA, TAC, and Ferric Reducing Ability of Plasma (FRAP). The data were pooled to determine the effect size via weighted mean differences (WMDs) with 95% CI. The random-effects model was used to calculate the WMDs with 95% CIs for conducting the meta-analysis. The statistical heterogeneity of included studies was assessed by the Q test and I2 statistics. Statistical difference in heterogeneity existed if P-value < 0.1 and I2 is greater than 50% (Higgins and Thompson, 2002). To identify the possible sources of heterogeneity in the included studies, sub-group analysis was performed.
Funnel plot and asymmetry tests, including Begg’s rank correlation test and Egger’s regression test were used for assessment of potential publication bias. Sensitivity analysis was conducted to examine effect of any study on the overall effect size. All of the analyses were performed using STATA version 14.0 (Stata Corp., College Station, TX, USA). A P-value < 0.05 was considered to be statistically significant unless otherwise specified.
Study selection: Flow chart of studies selection process is presented in Figure 1. According to the search designs from electronic medical databases, 1677 articles were found. 1580 article reminded after removing of duplicated. Eighteen article were removed for animal and cell line studies (n=1334), observational studies (n=79), review studies (n=60), clinical trials not about quercetin on OS (n=29), other articles (n=78). Eventually, 8 eligible studies included in this meta-analysis.
Study selection: Flow chart of studies selection process is presented in Figure 1. According to the search designs from electronic medical databases, 1677 articles were found. 1580 article reminded after removing of duplicated. Eighteen article were removed for animal and cell line studies (n=1334), observational studies (n=79), review studies (n=60), clinical trials not about quercetin on OS (n=29), other articles (n=78). Eventually, 8 eligible studies included in this meta-analysis.
Quality assessment of the studies: The assessment of quality for the included articles is summarized in Table 1. Briefly, all studies were categorized as low risk of bias for incomplete outcome data, random sequence generation, selective reporting, and blinding of participants and personnel. Two studies were considered low risk of bias for allocation concealment and the remaining did not express any method for allocation concealment, so were regarded as unclear risk of bias. Blinding of outcome assessment was unclear in five studies. Five included studies were at least 1 of the 6 key domains unclear risk of bias, thus the overall quality was considered to be unclear and two studies were for all key domains low risk of bias, therefore their overall quality became low risk of bias.
Characteristics of studies: The details of the 8 included studies are presented in Table 2. Studies were listed based on the following information: country, age(y), gender, sample size (intervention), RCT design, intervention name, quercetin dosage, name control, duration, outcome, and health status of participants. Studies were published from 2007 to 2020 and sample size ranged from 8 to 668 participants. Cross-over design was in two studies. The intervention duration in the trials was
between 1 to 84 days. The dose of quercetin in the intervention groups was from 500 to 2000 mg/day. Three and four studies were conducted in Iran and USD, respectively, and one study in Netherlands.
Results
Effect of quercetin supplementation on TAC level: Overall, 3 clinical trials examined the effect of Quercetin supplementation on TAC. The analysis demonstrated that quercetin supplementation had a no significant effect on TAC levels (WMD = 0.37 mmol/l; 95% confidence interval CI: -0.380, 0.454 mmol/l P = 0.864) and there was a significant heterogeneity between studies (Q statistic = 8.34, Cochrane Q test, P = 0.015, I2 = 76%, Figure 2).
Effect of quercetin supplementation on MDA: Four studies assessed the effect of quercetin supplementation on MDA and the meta-analysis showed no significant effect in the MDA level (WMD = 0.12 mmol/l; 95% confidence interval (CI): -0.106, 0.345 mmol/l; P = 0.298]. However, heterogeneity was low between studies (Q statistic = 1.62, Cochrane Q test, P = 0.654, I2 = 0%, Figure 3).
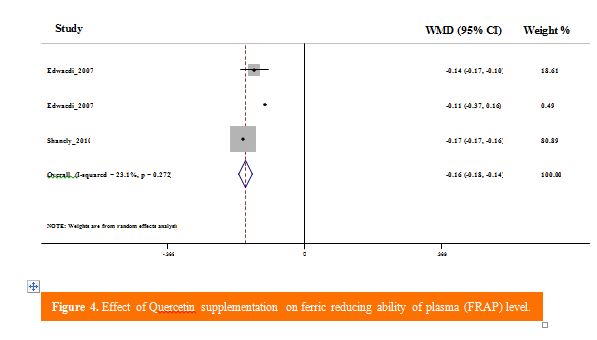
Effect of quercetin supplementation on FRAP: Three studies were included in the meta-analysis. The analysis illustrated that quercetin supplementation significantly increased FRAP in adults (WMD = -0.159 mmol/l, 95% confidence interval (CI): -0.178, -0.141, P ≤ 0.001). However, heterogeneity was low between studies (Q statistic = 2.6, Cochrane Q test, P = 0.272, I2 = 23.1%, Figure 4).
Sensitivity analysis and publication bias: The removal of the studies, one by one, did not considerably change the effect of quercetin consumption on TAC, MDA or FRAP. Mction coefficient, using 0.2 and 0.8 did not change the outcomes.
Although a slight asymmetry was seen in Begg’s funnel plots. There was no evidence for the attendance of publication bias using statistical asymmetry tests: TAC (Begg’s test, P = 1.00; Egger’s test, P = 0.834), MAD (Begg’s test, P = 1.00; Egger’s test, P = 0.30), FRAP (Begg’s test, P = 1.00; Egger’s test, P = 0.340). Results of funnel plot for Begg test are respectively shown in Figure 5, 6, and 7 for TAC, MDA, and FRAP.
|
( |
|
|
|
|
| Table 1. Risk of bias assessment according to the Cochrane collaboration tool. | |||||||
| First author (year) | Random sequence (generation) |
Allocation concealment |
Blinding of participants and personnel |
Blinding of outcome assessment |
Incomplete Outcome data |
Selective reporting |
Summary of overall assessment |
| Randi L. et al. (2007) | L | U | L | U | L | L | U |
| R. Andrew Shanel Y et al. (2010) | L | U | L | L | L | U | |
| Agnes W. Boot et al. (2011) | L | U | L | U | L | L | U |
| Fatemeh Javadi et al. (2012) | L | U | L | U | L | L | U |
| Shane D Scholten et al. (2013) | L | U | L | U | L | L | U |
| Zohreh Sajadi Hezaveh et al. (2019) | L | L | L | L | L | L | |
| Fereshteh Dehghani et al. ( 2020) | L | L | L | L | L | L | L |
| Table 2. General characteristics of the included studies. | ||||||||||
| Status of health | Duration (weak) | Outcome | con | Dosage of quercetin (mg/day) |
Sample size (int) |
Gender | Age (y) | Country | First author (year) | |
| CON | INT | |||||||||
| Major beta‑thalassemia |
12 |
MDA Before: 16.87 ± 5.23 mg/dl After: 16.37 ± 5.33 µmol/l TAC Before:2.81 ± 0.79 mmol/l After: 2.86 ± 0.92 mmol/l |
MDA Before: 18/59 ± 6.21µmol/l After: 17.31± 7.19 µmol/l TAC Before: 2.89 ± 0.74mmol/l After: 3.44 ± 0.97mmol/l |
Starch |
500 |
71(40) |
F/M |
Range: 18-40 |
Iran |
Zohreh Sajadi Hezaveh, et al. (2019) |
| Rheumatoid arthritis (RA) |
8 |
MDA Before: 4.71 ± 1.26 µmol/l After: 5.25 ± 1.98 µmol/l TAC Before: 0.34 ± 0.15 mmol/l After: 0.34 ± 0.08 mmol/L |
MDA Before: 3.79 ± 0.98 µmol/l After: 3.98 ± 0.10 µmol/l TAC Before: 0.36 ± 0.14 mmol/l After: 0.32 ± 0.08 mmol/l |
Lactose |
500 |
40(20) |
F |
Range: 19‑70 |
Iran |
Fatemeh Javadi, et al. (2014) |
| Healthy |
6 |
MDA Before: 12.33 ± 15.1 µmol/l After: 11.12 ± 1.78 µmol/l TAC Before: 3.3 ± 0.7 nmol/mg After: 3.49 ± 0.2 nmol/mg |
MDA Before: 11.78 ± 1.51 µmol/l After: 10.68 ± 0.82 µmol/l TAC Before: 3.22 ± 0.12 nmol/mg After: 2.96 ± 0.29 nmol/mg |
Not reported |
1000 |
8(5) |
M |
Range: 18-39 |
USA |
Shane D Scholten, et al. (2013) |
| Sarcoidosis | 1 day | Not reported | MDA Before: 0.37 ± 0.07 µmol/l |
Not reported | 2000 | 18(12) | F/M | Mean: 45 |
Netherlands | Agnes W. Boots et al. (2011) |
| Post-MI |
8 |
TAC Before: 0.55 ± 2 mmol/l After: 0.55 ± 0.6 mmol/l |
TAC Before: 0.62 ± 1.94 mmol/l After: 0.65 ± 1.94 mmol/l |
Lactose, cellulose, and starch |
500 |
88(44) |
F/M |
Range: 35–65 |
Iran |
Fereshteh Dehghani- 2020 |
| Non-institutionalized and pregnant and lactating women were excluded |
12 |
FRAP Before: 0.592 ± 0.012 mol/l After: 0.585 ± 0.014 mmol/l |
FRAP Before: 0.596 ± 0.013 mol/l After: 0.531± 0.011mmol/l |
250 mg vit C+10 mg niacin |
1000 +250 mg vit C+10 mg niacin |
668(333) |
F/M |
Range: 18-85 |
USA |
R. Andrew Shanely, et al. (2009) |
Discussion
The finding of the current study showed that quercetin supplementation had no significant effect on TAC levels, but the overall result represented a significant increase in FRAP levels in adults. However, heterogeneity was not high between these studies. Also, MDA level did not markedly change with this supplementation. However, sensitivity analysis did not represent any sensitivity to the included studies.
OS plays a key role in the pathogenesis of many common diseases, such as diabetes, cardiovascular diseases, obesity and cancer (Halliwell, 2000). It might account for progressive damage DNA, proteins, and lipids. In fact, it is produced in the body following ageing processes or during an acute inflammatory response. Therefore, there is a link between OS and inflammation (Basu, 2008, Finkel, 2003).
Many surveys have been carried out over the effect of quercetin on different factors which have shown controversial results. A recent systematic review and meta-analysis assessed the impact of quercetin supplementation on inflammatory markers and lipid profiles among patients with metabolic syndrome and related disorders, which demonstrated that quercetin supplementation considerably diminished total-cholesterol, low density lipoprotein cholesterol (LDL-c), and CRP levels, while did not affect triglycerides, high density lipoprotein cholesterol (HDL-c), IL-6, and TNF-α (Tabrizi et al., 2020). In contrast, another meta-analysis did not report any relevant effects of quercetin on peripheral CRP, IL-6, and TNF-α, although circulating CRP significantly decreased (Ou et al., 2020). The results of a recently published meta-analysis showed that the effect of quercetin on plasma lipid profiles, blood pressure, and glucose levels significantly reduced both systolic and diastolic blood pressure, but not in other markers of lipid profiles and glucose concentrations (Huang et al., 2020).
Also, the effect of quercetin, as an adenosine-receptor antagonist, on the reduction of OS was evaluated via inhibition of the enzyme xanthine oxidase (XO) that did not change after repeated sprints (Abbey and Rankin, 2011).
Another survey has assessed the impact of quercetin on endothelin-1 and OS after nitric oxide production by the measurement of S-nitrosothiols, nitrite and nitrate concentrations and F2-isoprostanes, respectively. Although, urinary endothelin-1 concentration significantly decreased by quercetin, the level of plasma or urinary F2-isoprostane concentrations did not change markedly, and showed no significant effect of quercetin on OS (Loke et al., 2008). The effect of quercetin on plasma antioxidant levels and increase in exercise-induced oxidative damage in forty athletes has been investigated through measurement of F2-isoprostanes, FRAP, nitrite, trolox equivalent antioxidant capacity, and CRP. Despite demonstrating in-vitro potent antioxidant actions of quercetin in previous studies, the results of this study represented no protection of chronic quercetin ingestion from inflammation and exercise-induced OS (McAnulty et al., 2008).
Subsequently, these controversial results can be impacted by several factors, including different dosage and duration of supplementary treatment, sample size of surveys, diverse status of subjects' health in the beginning and initial levels of OS markers (Haghighat et al., 2013, Sangsefidi et al., 2020). A previous study has shown that F2-isoprostanes and FRAP differed significantly between the obese and normal weight subjects, although subgroup analyses for body mass index (BMI) did not represent any significant difference (Shanely et al., 2010). The role of polyphenols can change between antioxidants and pro-oxidants according to the concentration of polyphenols and free radical sources, which consequently can act as either anti-inflammatory or pro-inflammatory compounds (Cao et al., 1997, Di et al., 2008).
The role of ROS and its abnormal regulation
in pathological conditions, encompassing inflammation, cancer, angiogenesis, atherosclerosis, and aging is undeniable (Gibellini et al., 2010). On the other hand, protective role of quercetin against inflammation, apoptosis and OS has been proved in many studies (Ghosh et al., 2009, Harwood et al., 2007, Liu et al., 2010). There are several mechanisms by which quercetin can link to growth, cell survival, apoptosis, and inflammation, such as protein kinase B, mitogen-activated protein kinases (MAPKs), phosphoinositol-3-kinase, NK-κB, and COX-2 (Granado-Serrano et al., 2006, Lee et al., 2007, Raja et al., 2017).
Using advanced search strategy, lack of linguistic restrictions in the search process, quality assessment basis on the Cochrane criteria as well as low heterogeneity and low publication bias were among the advantages of this study. On the other hand, there are some limitations, including low number of included trials and low subgroup analysis according to duration and dosage of supplementation.
Conclusion
As a result, the current study represents that the supplementation with quercetin had no significant effect on TAC and MDA levels but increased FRAP. More surveys with bigger sample sizes and high quality are needed to illustrate the effective role of quercetin in the reduction of ROS.
Acknowledgments
We acknowledge the contribution of the co-researchers.
Authors’ contributions
Ahmadi Vasmehjani A conceived the idea. Darabi Z and Ahmadi Vasmehjani A prepared the proposal. Hosseinzadeh M, Darabi Z, Ahmadi Vasmehjani A obtained ethical approvals, provided data extraction. Sangsefidi ZS and Abdollahi were analysis of article. Yaghoubi F, Ahmadi Vasmehjani A wrote the manuscript. Authors read and approved the final manuscript.
Competing interests
The authors have declared no competing interests.
Funding
The present study was not founded.
References
Abbey EL & Rankin JW 2011. Effect of quercetin supplementation on repeated-sprint performance, xanthine oxidase activity, and inflammation. International journal of sport nutrition and exercise metabolism. 21 (2): 91-96.
Barja G 2013. Updating the mitochondrial free radical theory of aging: an integrated view, key aspects, and confounding concepts. Antioxidants & redox signaling. 19 (12): 1420-1445.
Basu S 2008. F2-isoprostanes in human health and diseases: from molecular mechanisms to clinical implications. Antioxidants & redox signaling. 10 (8): 1405-1434.
Bazzucchi I, et al. 2019. The effects of quercetin supplementation on eccentric exercise-induced muscle damage. Nutrients. 11 (1): 205.
Birben E, Sahiner UM, Sackesen C, Erzurum S & Kalayci O 2012. Oxidative stress and antioxidant defense. World allergy organization journal. 5 (1): 9-19.
Boots AW, Drent M, de Boer VC, Bast A & Haenen GR 2011. Quercetin reduces markers of oxidative stress and inflammation in sarcoidosis. Clinical nutrition. 30 (4): 506-512.
Brüll V, et al. 2015. Effects of a quercetin-rich onion skin extract on 24 h ambulatory blood pressure and endothelial function in overweight-to-obese patients with (pre-) hypertension: a randomised double-blinded placebo-controlled cross-over trial. British journal of nutrition. 114 (8): 1263-1277.
Cao G, Sofic E & Prior RL 1997. Antioxidant and prooxidant behavior of flavonoids: structure-activity relationships. Free radical biology and medicine. 22 (5): 749-760.
Di AC, et al. 2008. Regular consumption of dark chocolate is associated with low serum concentrations of C-reactive protein in a healthy Italian population. Journal of nutrition. 138 (10): 1939-1945.
Egert S, et al. 2009. Quercetin reduces systolic blood pressure and plasma oxidised low-density lipoprotein concentrations in overweight subjects with a high-cardiovascular disease risk phenotype: a double-blinded, placebo-controlled cross-over study. British journal of nutrition. 102 (7): 1065-1074.
Egert S, et al. 2008. Daily quercetin supplementation dose-dependently increases plasma quercetin concentrations in healthy humans. Journal of nutrition. 138 (9): 1615-1621.
Finkel T 2003. Oxidant signals and oxidative stress. Current opinion in cell biology. 15 (2): 247-254.
Ghosh A, Mandal AK, Sarkar S, Panda S & Das N 2009. Nanoencapsulation of quercetin enhances its dietary efficacy in combating arsenic-induced oxidative damage in liver and brain of rats. Life sciences. 84 (3-4): 75-80.
Gibellini L, et al. 2010. Interfering with ROS metabolism in cancer cells: the potential role of quercetin. Cancers. 2 (2): 1288-1311.
Granado-Serrano AB, Martín MA, Bravo L, Goya L & Ramos S 2006. Quercetin induces apoptosis via caspase activation, regulation of Bcl-2, and inhibition of PI-3-kinase/Akt and ERK pathways in a human hepatoma cell line (HepG2). Journal of nutrition. 136 (11): 2715-2721.
Haghighat N, et al. 2013. The effects of dark chocolate on lipid profile, apo-lipoprotein A-1, apo-lipoprotein B and inflammation in type-2 diabetic patients: A randomized clinical trial. Iranian journal of nutrition sciences & food technology. 8 (2): 21-30.
Halliwell B 2000. Lipid peroxidation, antioxidants and cardiovascular disease: how should we move forward? Cardiovascular research. 47 (3): 410-418.
Harwood M, et al. 2007. A critical review of the data related to the safety of quercetin and lack of evidence of in vivo toxicity, including lack of genotoxic/carcinogenic properties. Food
and chemical toxicology. 45 (11): 2179-2205.
Higgins JP & Thompson SG 2002. Quantifying heterogeneity in a meta‐analysis. Statistics in medicine. 21 (11): 1539-1558.
Huang H, Liao D, Dong Y & Pu R 2020. Effect of quercetin supplementation on plasma lipid profiles, blood pressure, and glucose levels: a systematic review and meta-analysis. Nutrition reviews.
Lee EJ, et al. 2007. Cyclooxygenase-2 promotes cell proliferation, migration and invasion in U2OS human osteosarcoma cells. Experimental & molecular medicine. 39 (4): 469-476.
Liberati A, et al. 2009. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. Journal of clinical epidemiology. 62 (10): e1-e34.
Linke A, et al. 2005. Antioxidative effects of exercise training in patients with chronic heart failure: increase in radical scavenger enzyme activity in skeletal muscle. Circulation. 111 (14): 1763-1770.
Liu C-M, Ma J-Q & Sun Y-Z 2010. Quercetin protects the rat kidney against oxidative stress-mediated DNA damage and apoptosis induced by lead. Environmental toxicology and pharmacology. 30 (3): 264-271.
Loke WM, et al. 2008. Pure dietary flavonoids quercetin and (−)-epicatechin augment nitric oxide products and reduce endothelin-1 acutely in healthy men. American journal of clinical nutrition. 88 (4): 1018-1025.
Lorzadeh E, Ramezani-Jolfaie N, Mohammadi M, Khoshbakht Y & Salehi-Abargouei A 2019. The effect of hesperidin supplementation on inflammatory markers in human adults: a systematic review and meta-analysis of randomized controlled clinical trials. Chemico-biological interactions. 307: 8-15.
McAnulty SR, et al. 2008. Chronic quercetin ingestion and exercise-induced oxidative damage and inflammation. Applied physiology, nutrition, and metabolism. 33 (2): 254-262.
Ou Q, Zheng Z, Zhao Y & Lin W 2020. Impact of quercetin on systemic levels of inflammation: A meta-analysis of randomised controlled human trials. International Journal of Food Sciences and Nutrition. 71 (2): 152-163.
Raja SB, et al. 2017. Differential cytotoxic activity of Quercetin on colonic cancer cells depends on ROS generation through COX-2 expression. Food and chemical toxicology. 106: 92-106.
Riva A, Ronchi M, Petrangolini G, Bosisio S & Allegrini P 2019. Improved Oral Absorption of Quercetin from Quercetin Phytosome®, a New Delivery System Based on Food Grade Lecithin. European journal of drug metabolism and pharmacokinetics. 44 (2): 169-177.
Sangsefidi ZS, Yaghoubi F, Hajiahmadi S & Hosseinzadeh M 2020. The effect of coenzyme Q10 supplementation on oxidative stress: A systematic review and meta‐analysis of randomized controlled clinical trials. Food science & nutrition. 8 (4): 1766-1776.
Scholten SD & Sergeev IN 2013. Long-term quercetin supplementation reduces lipid peroxidation but does not improve performance in endurance runners. Open access journal of sports medicine. 4: 53.
Sepidarkish M, et al. 2019. The effect of vitamin D supplementation on oxidative stress parameters: a systematic review and meta-analysis of clinical trials. Pharmacological research. 139: 141-152.
Shanely RA, et al. 2010. Quercetin supplementation does not alter antioxidant status in humans. Free radical research. 44 (2): 224-231.
Sties SW, et al. 2018. Influence of exercise on oxidative stress in patients with heart failure. Heart failure reviews. 23 (2): 225-235.
Tabrizi R, et al. 2020. The effects of quercetin supplementation on lipid profiles and inflammatory markers among patients with metabolic syndrome and related disorders: A systematic review and meta-analysis of randomized controlled trials. Critical reviews in food science and nutrition. 60 (11): 1855-1868.
van't Erve TJ 2018. Strategies to decrease oxidative stress biomarker levels in human medical conditions: A meta-analysis on 8-iso-prostaglandin F2α. Redox biology. 17: 284-296.
OS plays a key role in the pathogenesis of many common diseases, such as diabetes, cardiovascular diseases, obesity and cancer (Halliwell, 2000). It might account for progressive damage DNA, proteins, and lipids. In fact, it is produced in the body following ageing processes or during an acute inflammatory response. Therefore, there is a link between OS and inflammation (Basu, 2008, Finkel, 2003).
Many surveys have been carried out over the effect of quercetin on different factors which have shown controversial results. A recent systematic review and meta-analysis assessed the impact of quercetin supplementation on inflammatory markers and lipid profiles among patients with metabolic syndrome and related disorders, which demonstrated that quercetin supplementation considerably diminished total-cholesterol, low density lipoprotein cholesterol (LDL-c), and CRP levels, while did not affect triglycerides, high density lipoprotein cholesterol (HDL-c), IL-6, and TNF-α (Tabrizi et al., 2020). In contrast, another meta-analysis did not report any relevant effects of quercetin on peripheral CRP, IL-6, and TNF-α, although circulating CRP significantly decreased (Ou et al., 2020). The results of a recently published meta-analysis showed that the effect of quercetin on plasma lipid profiles, blood pressure, and glucose levels significantly reduced both systolic and diastolic blood pressure, but not in other markers of lipid profiles and glucose concentrations (Huang et al., 2020).
Also, the effect of quercetin, as an adenosine-receptor antagonist, on the reduction of OS was evaluated via inhibition of the enzyme xanthine oxidase (XO) that did not change after repeated sprints (Abbey and Rankin, 2011).
Another survey has assessed the impact of quercetin on endothelin-1 and OS after nitric oxide production by the measurement of S-nitrosothiols, nitrite and nitrate concentrations and F2-isoprostanes, respectively. Although, urinary endothelin-1 concentration significantly decreased by quercetin, the level of plasma or urinary F2-isoprostane concentrations did not change markedly, and showed no significant effect of quercetin on OS (Loke et al., 2008). The effect of quercetin on plasma antioxidant levels and increase in exercise-induced oxidative damage in forty athletes has been investigated through measurement of F2-isoprostanes, FRAP, nitrite, trolox equivalent antioxidant capacity, and CRP. Despite demonstrating in-vitro potent antioxidant actions of quercetin in previous studies, the results of this study represented no protection of chronic quercetin ingestion from inflammation and exercise-induced OS (McAnulty et al., 2008).
Subsequently, these controversial results can be impacted by several factors, including different dosage and duration of supplementary treatment, sample size of surveys, diverse status of subjects' health in the beginning and initial levels of OS markers (Haghighat et al., 2013, Sangsefidi et al., 2020). A previous study has shown that F2-isoprostanes and FRAP differed significantly between the obese and normal weight subjects, although subgroup analyses for body mass index (BMI) did not represent any significant difference (Shanely et al., 2010). The role of polyphenols can change between antioxidants and pro-oxidants according to the concentration of polyphenols and free radical sources, which consequently can act as either anti-inflammatory or pro-inflammatory compounds (Cao et al., 1997, Di et al., 2008).
The role of ROS and its abnormal regulation
in pathological conditions, encompassing inflammation, cancer, angiogenesis, atherosclerosis, and aging is undeniable (Gibellini et al., 2010). On the other hand, protective role of quercetin against inflammation, apoptosis and OS has been proved in many studies (Ghosh et al., 2009, Harwood et al., 2007, Liu et al., 2010). There are several mechanisms by which quercetin can link to growth, cell survival, apoptosis, and inflammation, such as protein kinase B, mitogen-activated protein kinases (MAPKs), phosphoinositol-3-kinase, NK-κB, and COX-2 (Granado-Serrano et al., 2006, Lee et al., 2007, Raja et al., 2017).
Using advanced search strategy, lack of linguistic restrictions in the search process, quality assessment basis on the Cochrane criteria as well as low heterogeneity and low publication bias were among the advantages of this study. On the other hand, there are some limitations, including low number of included trials and low subgroup analysis according to duration and dosage of supplementation.
Conclusion
As a result, the current study represents that the supplementation with quercetin had no significant effect on TAC and MDA levels but increased FRAP. More surveys with bigger sample sizes and high quality are needed to illustrate the effective role of quercetin in the reduction of ROS.
Acknowledgments
We acknowledge the contribution of the co-researchers.
Authors’ contributions
Ahmadi Vasmehjani A conceived the idea. Darabi Z and Ahmadi Vasmehjani A prepared the proposal. Hosseinzadeh M, Darabi Z, Ahmadi Vasmehjani A obtained ethical approvals, provided data extraction. Sangsefidi ZS and Abdollahi were analysis of article. Yaghoubi F, Ahmadi Vasmehjani A wrote the manuscript. Authors read and approved the final manuscript.
Competing interests
The authors have declared no competing interests.
Funding
The present study was not founded.
References
Abbey EL & Rankin JW 2011. Effect of quercetin supplementation on repeated-sprint performance, xanthine oxidase activity, and inflammation. International journal of sport nutrition and exercise metabolism. 21 (2): 91-96.
Barja G 2013. Updating the mitochondrial free radical theory of aging: an integrated view, key aspects, and confounding concepts. Antioxidants & redox signaling. 19 (12): 1420-1445.
Basu S 2008. F2-isoprostanes in human health and diseases: from molecular mechanisms to clinical implications. Antioxidants & redox signaling. 10 (8): 1405-1434.
Bazzucchi I, et al. 2019. The effects of quercetin supplementation on eccentric exercise-induced muscle damage. Nutrients. 11 (1): 205.
Birben E, Sahiner UM, Sackesen C, Erzurum S & Kalayci O 2012. Oxidative stress and antioxidant defense. World allergy organization journal. 5 (1): 9-19.
Boots AW, Drent M, de Boer VC, Bast A & Haenen GR 2011. Quercetin reduces markers of oxidative stress and inflammation in sarcoidosis. Clinical nutrition. 30 (4): 506-512.
Brüll V, et al. 2015. Effects of a quercetin-rich onion skin extract on 24 h ambulatory blood pressure and endothelial function in overweight-to-obese patients with (pre-) hypertension: a randomised double-blinded placebo-controlled cross-over trial. British journal of nutrition. 114 (8): 1263-1277.
Cao G, Sofic E & Prior RL 1997. Antioxidant and prooxidant behavior of flavonoids: structure-activity relationships. Free radical biology and medicine. 22 (5): 749-760.
Di AC, et al. 2008. Regular consumption of dark chocolate is associated with low serum concentrations of C-reactive protein in a healthy Italian population. Journal of nutrition. 138 (10): 1939-1945.
Egert S, et al. 2009. Quercetin reduces systolic blood pressure and plasma oxidised low-density lipoprotein concentrations in overweight subjects with a high-cardiovascular disease risk phenotype: a double-blinded, placebo-controlled cross-over study. British journal of nutrition. 102 (7): 1065-1074.
Egert S, et al. 2008. Daily quercetin supplementation dose-dependently increases plasma quercetin concentrations in healthy humans. Journal of nutrition. 138 (9): 1615-1621.
Finkel T 2003. Oxidant signals and oxidative stress. Current opinion in cell biology. 15 (2): 247-254.
Ghosh A, Mandal AK, Sarkar S, Panda S & Das N 2009. Nanoencapsulation of quercetin enhances its dietary efficacy in combating arsenic-induced oxidative damage in liver and brain of rats. Life sciences. 84 (3-4): 75-80.
Gibellini L, et al. 2010. Interfering with ROS metabolism in cancer cells: the potential role of quercetin. Cancers. 2 (2): 1288-1311.
Granado-Serrano AB, Martín MA, Bravo L, Goya L & Ramos S 2006. Quercetin induces apoptosis via caspase activation, regulation of Bcl-2, and inhibition of PI-3-kinase/Akt and ERK pathways in a human hepatoma cell line (HepG2). Journal of nutrition. 136 (11): 2715-2721.
Haghighat N, et al. 2013. The effects of dark chocolate on lipid profile, apo-lipoprotein A-1, apo-lipoprotein B and inflammation in type-2 diabetic patients: A randomized clinical trial. Iranian journal of nutrition sciences & food technology. 8 (2): 21-30.
Halliwell B 2000. Lipid peroxidation, antioxidants and cardiovascular disease: how should we move forward? Cardiovascular research. 47 (3): 410-418.
Harwood M, et al. 2007. A critical review of the data related to the safety of quercetin and lack of evidence of in vivo toxicity, including lack of genotoxic/carcinogenic properties. Food
and chemical toxicology. 45 (11): 2179-2205.
Higgins JP & Thompson SG 2002. Quantifying heterogeneity in a meta‐analysis. Statistics in medicine. 21 (11): 1539-1558.
Huang H, Liao D, Dong Y & Pu R 2020. Effect of quercetin supplementation on plasma lipid profiles, blood pressure, and glucose levels: a systematic review and meta-analysis. Nutrition reviews.
Lee EJ, et al. 2007. Cyclooxygenase-2 promotes cell proliferation, migration and invasion in U2OS human osteosarcoma cells. Experimental & molecular medicine. 39 (4): 469-476.
Liberati A, et al. 2009. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. Journal of clinical epidemiology. 62 (10): e1-e34.
Linke A, et al. 2005. Antioxidative effects of exercise training in patients with chronic heart failure: increase in radical scavenger enzyme activity in skeletal muscle. Circulation. 111 (14): 1763-1770.
Liu C-M, Ma J-Q & Sun Y-Z 2010. Quercetin protects the rat kidney against oxidative stress-mediated DNA damage and apoptosis induced by lead. Environmental toxicology and pharmacology. 30 (3): 264-271.
Loke WM, et al. 2008. Pure dietary flavonoids quercetin and (−)-epicatechin augment nitric oxide products and reduce endothelin-1 acutely in healthy men. American journal of clinical nutrition. 88 (4): 1018-1025.
Lorzadeh E, Ramezani-Jolfaie N, Mohammadi M, Khoshbakht Y & Salehi-Abargouei A 2019. The effect of hesperidin supplementation on inflammatory markers in human adults: a systematic review and meta-analysis of randomized controlled clinical trials. Chemico-biological interactions. 307: 8-15.
McAnulty SR, et al. 2008. Chronic quercetin ingestion and exercise-induced oxidative damage and inflammation. Applied physiology, nutrition, and metabolism. 33 (2): 254-262.
Ou Q, Zheng Z, Zhao Y & Lin W 2020. Impact of quercetin on systemic levels of inflammation: A meta-analysis of randomised controlled human trials. International Journal of Food Sciences and Nutrition. 71 (2): 152-163.
Raja SB, et al. 2017. Differential cytotoxic activity of Quercetin on colonic cancer cells depends on ROS generation through COX-2 expression. Food and chemical toxicology. 106: 92-106.
Riva A, Ronchi M, Petrangolini G, Bosisio S & Allegrini P 2019. Improved Oral Absorption of Quercetin from Quercetin Phytosome®, a New Delivery System Based on Food Grade Lecithin. European journal of drug metabolism and pharmacokinetics. 44 (2): 169-177.
Sangsefidi ZS, Yaghoubi F, Hajiahmadi S & Hosseinzadeh M 2020. The effect of coenzyme Q10 supplementation on oxidative stress: A systematic review and meta‐analysis of randomized controlled clinical trials. Food science & nutrition. 8 (4): 1766-1776.
Scholten SD & Sergeev IN 2013. Long-term quercetin supplementation reduces lipid peroxidation but does not improve performance in endurance runners. Open access journal of sports medicine. 4: 53.
Sepidarkish M, et al. 2019. The effect of vitamin D supplementation on oxidative stress parameters: a systematic review and meta-analysis of clinical trials. Pharmacological research. 139: 141-152.
Shanely RA, et al. 2010. Quercetin supplementation does not alter antioxidant status in humans. Free radical research. 44 (2): 224-231.
Sties SW, et al. 2018. Influence of exercise on oxidative stress in patients with heart failure. Heart failure reviews. 23 (2): 225-235.
Tabrizi R, et al. 2020. The effects of quercetin supplementation on lipid profiles and inflammatory markers among patients with metabolic syndrome and related disorders: A systematic review and meta-analysis of randomized controlled trials. Critical reviews in food science and nutrition. 60 (11): 1855-1868.
van't Erve TJ 2018. Strategies to decrease oxidative stress biomarker levels in human medical conditions: A meta-analysis on 8-iso-prostaglandin F2α. Redox biology. 17: 284-296.
Type of article: review article |
Subject:
public specific
Received: 2021/05/27 | Published: 2022/11/19 | ePublished: 2022/11/19
Received: 2021/05/27 | Published: 2022/11/19 | ePublished: 2022/11/19
References
1. Abbey EL & Rankin JW 2011. Effect of quercetin supplementation on repeated-sprint performance, xanthine oxidase activity, and inflammation. International journal of sport nutrition and exercise metabolism. 21 (2): 91-96.
2. Barja G 2013. Updating the mitochondrial free radical theory of aging: an integrated view, key aspects, and confounding concepts. Antioxidants & redox signaling. 19 (12): 1420-1445.
3. Basu S 2008. F2-isoprostanes in human health and diseases: from molecular mechanisms to clinical implications. Antioxidants & redox signaling. 10 (8): 1405-1434.
4. Bazzucchi I, et al. 2019. The effects of quercetin supplementation on eccentric exercise-induced muscle damage. Nutrients. 11 (1): 205.
5. Birben E, Sahiner UM, Sackesen C, Erzurum S & Kalayci O 2012. Oxidative stress and antioxidant defense. World allergy organization journal. 5 (1): 9-19.
6. Boots AW, Drent M, de Boer VC, Bast A & Haenen GR 2011. Quercetin reduces markers of oxidative stress and inflammation in sarcoidosis. Clinical nutrition. 30 (4): 506-512.
7. Brüll V, et al. 2015. Effects of a quercetin-rich onion skin extract on 24 h ambulatory blood pressure and endothelial function in overweight-to-obese patients with (pre-) hypertension: a randomised double-blinded placebo-controlled cross-over trial. British journal of nutrition. 114 (8): 1263-1277.
8. Cao G, Sofic E & Prior RL 1997. Antioxidant and prooxidant behavior of flavonoids: structure-activity relationships. Free radical biology and medicine. 22 (5): 749-760.
9. Di AC, et al. 2008. Regular consumption of dark chocolate is associated with low serum concentrations of C-reactive protein in a healthy Italian population. Journal of nutrition. 138 (10): 1939-1945.
10. Egert S, et al. 2009. Quercetin reduces systolic blood pressure and plasma oxidised low-density lipoprotein concentrations in overweight subjects with a high-cardiovascular disease risk phenotype: a double-blinded, placebo-controlled cross-over study. British journal of nutrition. 102 (7): 1065-1074.
11. Egert S, et al. 2008. Daily quercetin supplementation dose-dependently increases plasma quercetin concentrations in healthy humans. Journal of nutrition. 138 (9): 1615-1621.
12. Finkel T 2003. Oxidant signals and oxidative stress. Current opinion in cell biology. 15 (2): 247-254.
13. Ghosh A, Mandal AK, Sarkar S, Panda S & Das N 2009. Nanoencapsulation of quercetin enhances its dietary efficacy in combating arsenic-induced oxidative damage in liver and brain of rats. Life sciences. 84 (3-4): 75-80.
14. Gibellini L, et al. 2010. Interfering with ROS metabolism in cancer cells: the potential role of quercetin. Cancers. 2 (2): 1288-1311.
15. Granado-Serrano AB, Martín MA, Bravo L, Goya L & Ramos S 2006. Quercetin induces apoptosis via caspase activation, regulation of Bcl-2, and inhibition of PI-3-kinase/Akt and ERK pathways in a human hepatoma cell line (HepG2). Journal of nutrition. 136 (11): 2715-2721.
16. Haghighat N, et al. 2013. The effects of dark chocolate on lipid profile, apo-lipoprotein A-1, apo-lipoprotein B and inflammation in type-2 diabetic patients: A randomized clinical trial. Iranian journal of nutrition sciences & food technology. 8 (2): 21-30.
17. Halliwell B 2000. Lipid peroxidation, antioxidants and cardiovascular disease: how should we move forward? Cardiovascular research. 47 (3): 410-418.
18. Harwood M, et al. 2007. A critical review of the data related to the safety of quercetin and lack of evidence of in vivo toxicity, including lack of genotoxic/carcinogenic properties. Food and chemical toxicology. 45 (11): 2179-2205.
20. Higgins JP & Thompson SG 2002. Quantifying heterogeneity in a meta‐analysis. Statistics in medicine. 21 (11): 1539-1558.
21. Huang H, Liao D, Dong Y & Pu R 2020. Effect of quercetin supplementation on plasma lipid profiles, blood pressure, and glucose levels: a systematic review and meta-analysis. Nutrition reviews.
22. Lee EJ, et al. 2007. Cyclooxygenase-2 promotes cell proliferation, migration and invasion in U2OS human osteosarcoma cells. Experimental & molecular medicine. 39 (4): 469-476.
23. Liberati A, et al. 2009. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. Journal of clinical epidemiology. 62 (10): e1-e34.
24. Linke A, et al. 2005. Antioxidative effects of exercise training in patients with chronic heart failure: increase in radical scavenger enzyme activity in skeletal muscle. Circulation. 111 (14): 1763-1770.
25. Liu C-M, Ma J-Q & Sun Y-Z 2010. Quercetin protects the rat kidney against oxidative stress-mediated DNA damage and apoptosis induced by lead. Environmental toxicology and pharmacology. 30 (3): 264-271.
26. Loke WM, et al. 2008. Pure dietary flavonoids quercetin and (−)-epicatechin augment nitric oxide products and reduce endothelin-1 acutely in healthy men. American journal of clinical nutrition. 88 (4): 1018-1025.
27. Lorzadeh E, Ramezani-Jolfaie N, Mohammadi M, Khoshbakht Y & Salehi-Abargouei A 2019. The effect of hesperidin supplementation on inflammatory markers in human adults: a systematic review and meta-analysis of randomized controlled clinical trials. Chemico-biological interactions. 307: 8-15.
28. McAnulty SR, et al. 2008. Chronic quercetin ingestion and exercise-induced oxidative damage and inflammation. Applied physiology, nutrition, and metabolism. 33 (2): 254-262.
29. Ou Q, Zheng Z, Zhao Y & Lin W 2020. Impact of quercetin on systemic levels of inflammation: A meta-analysis of randomised controlled human trials. International Journal of Food Sciences and Nutrition. 71 (2): 152-163.
30. Raja SB, et al. 2017. Differential cytotoxic activity of Quercetin on colonic cancer cells depends on ROS generation through COX-2 expression. Food and chemical toxicology. 106: 92-106.
31. Riva A, Ronchi M, Petrangolini G, Bosisio S & Allegrini P 2019. Improved Oral Absorption of Quercetin from Quercetin Phytosome®, a New Delivery System Based on Food Grade Lecithin. European journal of drug metabolism and pharmacokinetics. 44 (2): 169-177.
32. Sangsefidi ZS, Yaghoubi F, Hajiahmadi S & Hosseinzadeh M 2020. The effect of coenzyme Q10 supplementation on oxidative stress: A systematic review and meta‐analysis of randomized controlled clinical trials. Food science & nutrition. 8 (4): 1766-1776.
33. Scholten SD & Sergeev IN 2013. Long-term quercetin supplementation reduces lipid peroxidation but does not improve performance in endurance runners. Open access journal of sports medicine. 4: 53.
34. Sepidarkish M, et al. 2019. The effect of vitamin D supplementation on oxidative stress parameters: a systematic review and meta-analysis of clinical trials. Pharmacological research. 139: 141-152.
35. Shanely RA, et al. 2010. Quercetin supplementation does not alter antioxidant status in humans. Free radical research. 44 (2): 224-231.
36. Sties SW, et al. 2018. Influence of exercise on oxidative stress in patients with heart failure. Heart failure reviews. 23 (2): 225-235.
37. Tabrizi R, et al. 2020. The effects of quercetin supplementation on lipid profiles and inflammatory markers among patients with metabolic syndrome and related disorders: A systematic review and meta-analysis of randomized controlled trials. Critical reviews in food science and nutrition. 60 (11): 1855-1868.
38. van't Erve TJ 2018. Strategies to decrease oxidative stress biomarker levels in human medical conditions: A meta-analysis on 8-iso-prostaglandin F2α. Redox biology. 17: 284-296.
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
