
Mon, Jul 13, 2026
[Archive]
Volume 6, Issue 3 (Aug 2021)
JNFS 2021, 6(3): 226-231 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Humayun N, Bashir S, Khalid S. Comparison of Nutrients Intake among Pregnant Anemic & Non-Anemic Women. JNFS 2021; 6 (3) :226-231
URL: http://jnfs.ssu.ac.ir/article-1-334-en.html
URL: http://jnfs.ssu.ac.ir/article-1-334-en.html



Institute of Diet and Nutritional Sciences, Faculty of Allied Health Sciences, The University of Lahore, Pakistan.
Keywords: Nutrients intake, Pregnant anemic women, Low protein diet, Tea, recommended dietary allowance
Full-Text [PDF 466 kb]
(829 Downloads)
| Abstract (HTML) (3248 Views)
Introduction

Full-Text: (648 Views)
Comparison of Nutrients Intake among Pregnant Anemic & Non-Anemic Women
Nouf Humayun; BSc 1, Shahid Bashir; PhD 1 & Sidra Khalid; MPhil *1
1 Institute of Diet and Nutritional Sciences, Faculty of Allied Health Sciences, The University of Lahore, Pakistan.Nouf Humayun; BSc 1, Shahid Bashir; PhD 1 & Sidra Khalid; MPhil *1
| ARTICLE INFO | ABSTRACT | |
| ORIGINAL ARTICLE |
Background: Anemia, interpreted as a low blood hemoglobin values, was considered as a major health complication in the world. However, anemia in pregnancy is a global public health problem in the developing countries, posing high risk of adverse results for expecting mothers as well as their fetus. The aim of study was to compare nutrients' intake among pregnant anemic & non-anemic women. Methods: A comparative cross-sectional study was conducted at Sir Ganga Ram Hospital, Lahore over a period of 4 months. The data were collected from 150 pregnant women, including 75 anemic and 75 non-anemic women, through pre-tested questionnaire using non-probability convenient sampling method. Data were tabulated and analyzed with help of SPSS version 21.0. Results: Analysis revealed that 34% of women had carbohydrate intake between 0-150 g/day, 44% had protein intake less than 50 g daily, and 36% had daily fat intake between 0-100 g/day. Moreover, 46.7% of the pregnant women were vitamins deficient, 51% were minerals deficient, 52% were iron deficient, 54.7% consumed tea with their meals, 44% had vitamin B3 intake less than 10 mg, 48% had vitamin C intake less than 50 mg, 48% had vitamin A intake between 0-500 RAE, 42% had calcium intake between 0-500 mg, and 31% had iron intake between 0-10 mg. Conclusion: The findings showed that nutrient intake of anemic pregnant women was not sufficient in the protein rich diet; they had high consumption of tea with their meals. Their overall energy intake and micronutrients were less than the required as per recommended dietary allowance in pregnancy.
Key words: Nutrients intake; Pregnant anemic women; Low protein diet; Tea; recommended dietary allowance |
|
| Article history: Received: 23 Jul 2020 Revised: 20 Feb 2021 Accepted: 20 Feb 2021 |
||
| *Corresponding author: Sidrakhalid.uaf@gmail.com The University of Lahore, Main campus, 1-Km Defence road, Bhuptian chowk, Lahore Pakistan. Postal code: 8917945918 Tel: +92-3347498338 |
Introduction
Anemia, interpreted as a low blood hemoglobin values, has been considered as a major health complication with critical outcomes in the developed and developing countries and additionally unfavorable effects on social and financial conditions (Stevens et al., 2013). Three mechanisms mainly lead to anemia: blood loss, when body is unable to produce enough red blood cells (erythropoiesis), and when red blood cells die (hemolysis). Genetic disorders and deficiency of certain nutrients are other contributors of anemia (Kassebaum, 2016). The most widely recognized reason of anemia is Iron deficiency, which is estimated to cause half of all instances of anemia. Because of their certain roles in synthesis of red blood cells and hemoglobin, deficiencies of vitamins A, riboflavin (B2), pyridoxine (B6), cobalamin (B12), C, D, E, folate, and copper can also lead to anemia (Balarajan et al., 2011).
People more susceptible to anemia include infants, children under five years, adolescents, females of reproductive age (both pregnant and non-pregnant), and elderly. For various reasons women are at a higher risk of having anemia: blood wastage every month with menstruation causes high iron losses and hence iron demand, during adolescence (high development and growth phase), and pregnancy incur additional requirements for iron (for their own growth and the growing fetus) (Torheim et al., 2010). It was estimated that about 1.3 billion people all over the world suffer from anemia, making it a standout amongst the most critical health problems globally. Many investigations showed the relationship of anemia with maternal diseases and death. Worldwide anemia adds to 20% of all maternal deaths, leading to premature deliveries, low birth weight, infant mortality, and mental impairment (Obai et al., 2016).
Anemia was also found prevalent (49%) among women in Pakistan according to the National Nutrition Survey (NNS) of 2011 (Bhutta et al., 2011). High prevalence of anemia was also reported among married women in urban (26%) and rural (47%) areas of Pakistan (Baig-Ansari et al., 2008). The prevalence of anemia among pregnant women living in urban areas is similar, ranging from 29% to 50% among pregnant women attending antenatal clinics in a large private, tertiary hospital in Karachi (Aziz-Karim et al., 1990). In the new born children, anemia was found to cause cognitive and behavioral dysfunction, low iron stores, and iron deficiency anemia (Lozoff et al., 2006). Lone FW revealed that infants of anemic mothers had 1.8 times higher chance of having low Appearance, Pulse, Grimace, Activity and Respiration (APGAR) score at the time of birth (Lone et al., 2004).
Rich dietary sources of iron include meat especially offal (organ meat), fish, eggs, poultry, and meat extracts. However, bread and flour, breakfast cereals, dark green vegetables, pulses, nuts, dried fruits like prunes, figs, and apricots are good sources of iron (Webster-Gandy et al., 2020). Dietary factors such as inadequate amount of iron rich foods, vitamin C rich foods (iron absorption enhancers), high amounts of iron inhibitors (e.g. tea, coffee, calcium rich foods) in the diet particularly at the time of meals lead to low bio-availability of dietary iron (Rasheed et al., 2008).
During pregnancy, an expanded danger of maternal and perinatal mortality and low size or weight at birth can be related with low hemoglobin values. Maternal and neonatal passing are a noteworthy reason for mortality in creating nations and cause deaths around the world (Abdelhafez and El-Soadaa, 2012, Zhang et al., 2009). In pregnancy, maternal anemia is viewed as a hazard factor for unfavorable outcomes. In developing countries, anemia is in charge of 40-60% of maternal passing. Directly or indirectly, anemia contributes to premature delivery, pre-eclampsia, infection, cardiac failure, and hemorrhage (Padmanabhan and Chandrakar, 2018).
The research was aimed to find out the nutrient intake causing anemia among pregnant females. Given the low level of knowledge regarding dietary practices, awareness should be increased through health education and regarding behaviors modification. In the case that these practices
and behaviors are not addressed on time, consequences of anemia on babies will increase, such as low body weight, malnutrition, delayed development, and still births. The purpose of this study was to compare the nutrient intake among pregnant females with and without anemia in order to highlight the effect of inappropriate dietary pattern and insufficient nutrients intake among pregnant anemic females.
Materials and Methods
Study design and participants: A comparative cross-sectional study design was used. Data were collected from females visiting the indoor and outdoor units of Gynae and Obstetrics department and vaccination center of Preventive Pediatrics department at Sir Ganga Ram Hospital, Lahore for a duration of 4 months in December 2018- March 2019. As a result, 150 pregnant women were enrolled in the study using non-probability convenient sampling technique. Pregnant females visiting the respective departments were selected for the follow-up routine checkup having biochemical profile. Later, the participants were categorized as anemic and non-anemic if they had Hb 8 g/dl or less and Hb above 8 g/dl, respectively.
Measurements: Data were collected via self-structured questionnaire regarding their demographics, medical history, food frequency questionnaire (FFQ) (Willett, 1998), and 24-hour recall. After receiving the written informed consent forms, data were collected by interview.
Ethical considerations: Ethical approval was taken from the Institutional Review Board (IRB) of the University of Lahore. All the rules and standards set by the committee were respected. Patients were pre-informed regarding the benefits of study, they were allowed to leave the study any time during interview. Their identities were kept anonyms. Prior written informed consents were taken from all the participating females.
Data analysis: The quantitative variables were assessed using mean ± SD and the qualitative variables were reported using frequencies and percentages. To analyze the data, SPSS version 21.0 was used. Nutrients from 24-hr dietary recall were derived with reference to the standard serving sizes using MS excel.
Results
The comparison of demographic profile showed insignificant association of patient’s age (P = 0.88) and significant association of age at the time of marriage (P = 0.02) between anemic and non-anemic females. Education (P = 0.001) and socio economic status (P = 0.001) also showed significant association with anemia. However, employment status showed insignificant association with anemia (P = 0.16) as shown in Table 1.
People more susceptible to anemia include infants, children under five years, adolescents, females of reproductive age (both pregnant and non-pregnant), and elderly. For various reasons women are at a higher risk of having anemia: blood wastage every month with menstruation causes high iron losses and hence iron demand, during adolescence (high development and growth phase), and pregnancy incur additional requirements for iron (for their own growth and the growing fetus) (Torheim et al., 2010). It was estimated that about 1.3 billion people all over the world suffer from anemia, making it a standout amongst the most critical health problems globally. Many investigations showed the relationship of anemia with maternal diseases and death. Worldwide anemia adds to 20% of all maternal deaths, leading to premature deliveries, low birth weight, infant mortality, and mental impairment (Obai et al., 2016).
Anemia was also found prevalent (49%) among women in Pakistan according to the National Nutrition Survey (NNS) of 2011 (Bhutta et al., 2011). High prevalence of anemia was also reported among married women in urban (26%) and rural (47%) areas of Pakistan (Baig-Ansari et al., 2008). The prevalence of anemia among pregnant women living in urban areas is similar, ranging from 29% to 50% among pregnant women attending antenatal clinics in a large private, tertiary hospital in Karachi (Aziz-Karim et al., 1990). In the new born children, anemia was found to cause cognitive and behavioral dysfunction, low iron stores, and iron deficiency anemia (Lozoff et al., 2006). Lone FW revealed that infants of anemic mothers had 1.8 times higher chance of having low Appearance, Pulse, Grimace, Activity and Respiration (APGAR) score at the time of birth (Lone et al., 2004).
Rich dietary sources of iron include meat especially offal (organ meat), fish, eggs, poultry, and meat extracts. However, bread and flour, breakfast cereals, dark green vegetables, pulses, nuts, dried fruits like prunes, figs, and apricots are good sources of iron (Webster-Gandy et al., 2020). Dietary factors such as inadequate amount of iron rich foods, vitamin C rich foods (iron absorption enhancers), high amounts of iron inhibitors (e.g. tea, coffee, calcium rich foods) in the diet particularly at the time of meals lead to low bio-availability of dietary iron (Rasheed et al., 2008).
During pregnancy, an expanded danger of maternal and perinatal mortality and low size or weight at birth can be related with low hemoglobin values. Maternal and neonatal passing are a noteworthy reason for mortality in creating nations and cause deaths around the world (Abdelhafez and El-Soadaa, 2012, Zhang et al., 2009). In pregnancy, maternal anemia is viewed as a hazard factor for unfavorable outcomes. In developing countries, anemia is in charge of 40-60% of maternal passing. Directly or indirectly, anemia contributes to premature delivery, pre-eclampsia, infection, cardiac failure, and hemorrhage (Padmanabhan and Chandrakar, 2018).
The research was aimed to find out the nutrient intake causing anemia among pregnant females. Given the low level of knowledge regarding dietary practices, awareness should be increased through health education and regarding behaviors modification. In the case that these practices
and behaviors are not addressed on time, consequences of anemia on babies will increase, such as low body weight, malnutrition, delayed development, and still births. The purpose of this study was to compare the nutrient intake among pregnant females with and without anemia in order to highlight the effect of inappropriate dietary pattern and insufficient nutrients intake among pregnant anemic females.
Materials and Methods
Study design and participants: A comparative cross-sectional study design was used. Data were collected from females visiting the indoor and outdoor units of Gynae and Obstetrics department and vaccination center of Preventive Pediatrics department at Sir Ganga Ram Hospital, Lahore for a duration of 4 months in December 2018- March 2019. As a result, 150 pregnant women were enrolled in the study using non-probability convenient sampling technique. Pregnant females visiting the respective departments were selected for the follow-up routine checkup having biochemical profile. Later, the participants were categorized as anemic and non-anemic if they had Hb 8 g/dl or less and Hb above 8 g/dl, respectively.
Measurements: Data were collected via self-structured questionnaire regarding their demographics, medical history, food frequency questionnaire (FFQ) (Willett, 1998), and 24-hour recall. After receiving the written informed consent forms, data were collected by interview.
Ethical considerations: Ethical approval was taken from the Institutional Review Board (IRB) of the University of Lahore. All the rules and standards set by the committee were respected. Patients were pre-informed regarding the benefits of study, they were allowed to leave the study any time during interview. Their identities were kept anonyms. Prior written informed consents were taken from all the participating females.
Data analysis: The quantitative variables were assessed using mean ± SD and the qualitative variables were reported using frequencies and percentages. To analyze the data, SPSS version 21.0 was used. Nutrients from 24-hr dietary recall were derived with reference to the standard serving sizes using MS excel.
Results
The comparison of demographic profile showed insignificant association of patient’s age (P = 0.88) and significant association of age at the time of marriage (P = 0.02) between anemic and non-anemic females. Education (P = 0.001) and socio economic status (P = 0.001) also showed significant association with anemia. However, employment status showed insignificant association with anemia (P = 0.16) as shown in Table 1.
Nutrient intakes of the pregnant women were estimated through 24-hour recall data. Mean value of energy intake in a day was 1429.7 ± 734 kcal for the anemic women and 1504.27 ± 736.4 kcal for non-anemic women; whereas, RDA of energy during pregnancy was 2200 Kcal. Mean value of daily carbohydrate intake of anemic women during 24 hours was 141.1 ± 80.4 g and non-anemic women intake was 135.4 ± 69.4 g; whereas, 175 g is considered as the RDA. The major reasons behind anemia among pregnant females included lower intake of protein (36.1 ± 20.0 g/day), which is approximately half of the RDA since protein is the building block of the cells and Hb; inadequate iron intake (8.9 ± 4.1 mg), which is highly lower than the RDA (as iron is the basic oxygen carrying unit of blood) and RDA (371.2 ± 173.8 mg); and intake of calcium, which helps oxygen carrying and iron absorption in blood.
Intake of other micronutrients was also not adequate, mean of vitamin A intake among anemic women was 605.1± 88.8 µg, while its RDA during pregnancy is 750-770 µg. Mean of Vitamin C intake was 20.0 ± 18.8 mg, whereas RDA is 80-85 mg. B1 and B2 intake means were 0.7 ± 0.3 mg and 0.5 ± 0.2 mg, respectively and their RDA during pregnancy is 1.4 mg. Mean intake of Niacin (B3) was 6.5 ± 5.2 mg and
its RDA was 18 mg during the pregnancy
(Table 2).
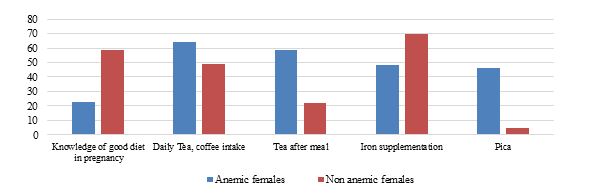
Dietary intake of the participants was recorded through FFQ. Findings showed that among the anemic group, only 23 females had the knowledge regarding balanced diet during pregnancy and 48 of them were taking iron supplements. However, among the basic reasons towards anemia, 64 anemic females were taking tea or coffee on daily basis, 59 were taking tea after meal, and 46 were having craving for pica (Figure 1).
Intake of other micronutrients was also not adequate, mean of vitamin A intake among anemic women was 605.1± 88.8 µg, while its RDA during pregnancy is 750-770 µg. Mean of Vitamin C intake was 20.0 ± 18.8 mg, whereas RDA is 80-85 mg. B1 and B2 intake means were 0.7 ± 0.3 mg and 0.5 ± 0.2 mg, respectively and their RDA during pregnancy is 1.4 mg. Mean intake of Niacin (B3) was 6.5 ± 5.2 mg and
its RDA was 18 mg during the pregnancy
(Table 2).
Dietary intake of the participants was recorded through FFQ. Findings showed that among the anemic group, only 23 females had the knowledge regarding balanced diet during pregnancy and 48 of them were taking iron supplements. However, among the basic reasons towards anemia, 64 anemic females were taking tea or coffee on daily basis, 59 were taking tea after meal, and 46 were having craving for pica (Figure 1).
| Figure 1. Comparison of dietary habits among anemic and non-anemic females |
| Table 1. Distribution of Age, age at the time of marriage, education, employment status, and socio-economic status of participants |
|||
| Variables | Anemic | Non anemic | P-valuea |
| Age (y) | 28.07 ± 4.34 | 28.17 ± 3.72 | 0.88 |
| Age at the time of marriage (y) | 22.47 ± 4.12 | 23.84 ± 3.06 | 0.02 |
| Education | |||
| Illiterate | 5 (7.4) | 0 (0.0) | 0.001 |
| Middle school | 16 (23.5) | 4 (4.9) | |
| Matriculation | 15 (22.1) | 8 (9.8) | |
| Intermediate | 14 (20.6) | 13 (15.9) | |
| Graduation and above | 18 (26.5) | 57 (69.5) | |
| Socio economic status | |||
| Lower class | 41 (60.3) | 20 (24.4) | 0.001 |
| Middle class | 18 (26.5) | 31 (37.8) | |
| Upper class | 9 (13.2) | 31 (37.8) | |
| Employment status | |||
| House work | 61 (89.7) | 67 (81.7) | 0.16 |
| Working women | 7 (10.3) | 15 (18.3) | |
| a: Chi-square test | |||
| Table 2. Comparison of nutrient intake among pregnant females | ||||
| Nutrients | Anemic | Non anemic | Recommended daily alowance | P-valuea |
| Energy (kcal) | 1429.7 ± 734.0 | 1504.27 ± 736.4 | 2200 | 0.53 |
| Carbohydrates (g) | 141.1 ± 80.4 | 135.4 ± 69.4 | 175 | 0.64 |
| Proteins (g) | 36.1 ± 20.0 | 53.94 ± 33.2 | 71 | <0.001 |
| Fats (g) | 80.2 ± 40.7 | 87.4 ± 50.3 | 65 | 0.34 |
| Iron (mg) | 8.9 ± 4.1 | 10.8 ± 6.9 | 27 | 0.04 |
| Calcium (mg) | 371.2 ± 173.8 | 430.0 ± 298.5 | 1000-1300 | 0.13 |
| Vitamin A (µg) | 605.1 ± 88.8 | 742.5 ± 919.4 | 750-770 | 0.22 |
| Vitamin C (mg) | 20.0 ± 18.8 | 26.0 ± 40.4 | 80-85 | 0.26 |
| Thiamin (mg) | 0.7 ± 0.3 | 0.7 ± 0.9 | 1.4 | 0.90 |
| Riboflavin (mg) | 0.5 ± 0.2 | 0.8 ± 1.0 | 1.4 | 0.01 |
| Niacin (mg) | 6.5 ± 5.2 | 7.4 ± 7.2 | 18 | 0.37 |
| a: Chi-square test | ||||
Discussion
Based on the findings, anemic females had significantly higher daily consumption of tea and coffee and majority of them were taking their tea serving with breakfast meal. Similar results were reported in previous study by Rai (Rai, 2018). On the contrary, Rai revealed that anemia was more common among women who consumed tea two or more than two times a day. The current study showed that 44.7% of the anemic patients had no knowledge regarding balance diet. Rai S also conducted a study and informed that not having enough knowledge of balance diet was a risk factor of developing anemia (Alzaheb and Al-Amer, 2017). A strong association between anemia and low consumption of beef, mutton, poultry, fish, and eggs was found. Findings revealed poor protein intake and nutritional status among the anemic expecting females as one of the major causative factors of anemia. Parallel results were found in studies by Alzaheb RA and Alaofè H (Alaofè et al., 2017, Alzaheb and Al-Amer, 2017), indicating diet deficiency in iron rich foods among pregnant females (Alaofè et al., 2017). Nik Rosmawati NH et al. carried out a research in 2009 in city of Terengganu, Malaysia and reported 57.4% prevalence of anemia with poor dietary and nutritional status(Nik Rosmawati et al., 2012). Parallel results were found in a number of previous studies (Alaofè et al., 2017, Nik Rosmawati et al., 2012). Current research showed that overall females had very low consumption of vitamin C rich foods in their diet, which is another risk factor of developing anemia, since vitamin C enhances the absorption of iron in body.
Conclusions
Findings showed that anemic females had higher tea consumption right after meals along with fewer intakes of protein, iron, and vitamin C as compared to the non-anemic females and RDA. Lack of education, lower literacy rate, less knowledge regarding balance diet, and improper iron supplementation among anemic females promoted higher prevalence of anemia in pregnancy.
Acknowledgments
We highly acknowledge the Preventive pediatrics department of Sir Ganga Ram Hospital, Lahore and Biostatistician (Ms. Humaira Waseem) of The University of Lahore for the guidance and cooperation.
Authors’ contributions
Humayun N conducted the study and collected the data. Bashir S supervised and designed the study, critical review of the manuscript and Khalid S literature search and manuscript write-up. All authors approved the final version of manuscript.
Conflict of interest
There is no conflict of interest to reveal.
Funding source
There was no funding source.
References
Abdelhafez AM & El-Soadaa SS 2012. Prevalence and risk factors of anemia among a sample of pregnant females attending primary health care centers in Makkah, Saudi Arabia. Pakistan journal of nutrition. 11 (12): 1113.
Alaofè H, Burney J, Naylor R & Taren D 2017. Prevalence of anaemia, deficiencies of iron and vitamin A and their determinants in rural women and young children: a cross-sectional study in Kalalé district of northern Benin. Public health nutrition. 20 (7): 1203-1213.
Alzaheb RA & Al-Amer O 2017. The prevalence of iron deficiency anemia and its associated risk factors among a sample of female university students in Tabuk, Saudi Arabia. Clinical medicine insights: women's health. 10: 1179562X17745088.
Aziz-Karim S, Khursheed M, Rizvi JH, Jafarey SN & Siddiqui RI 1990. Anaemia in pregnancy--a study of 709 women in Karachi. Tropical doctor. 20 (4): 184-185.
Baig-Ansari N, et al. 2008. Anemia prevalence and risk factors in pregnant women in an urban area of Pakistan. Food and nutrition bulletin. 29 (2): 132-139.
Balarajan Y, Ramakrishnan U, Özaltin E, Shankar AH & Subramanian S 2011. Anaemia in low-income and middle-income countries. lancet. 378 (9809): 2123-2135.
Bhutta Z, Soofi S, Zaidi S, Habib A & Hussain I 2011. National Nutrition Survey of Pakistan. Pakistan.
Kassebaum NJ 2016. The global burden of anemia. Hematology/Oncology clinics. 30 (2): 247-308.
Lone FW, Qureshi RN & Emanuel F 2004. Maternal anaemia and its impact on perinatal outcome. Tropical medicine & international health. 9 (4): 486-490.
Lozoff B, et al. 2006. Long-lasting neural and behavioral effects of iron deficiency in infancy. Nutrition reviews. 64 (suppl_2): S34-S43.
Nik Rosmawati N, Mohd Nazri S & Mohd Ismail I 2012. The rate and risk factors for anemia among pregnant mothers in Jerteh Terengganu, Malaysia. Journal of community medicine and health education. 2 (150): 2161-0711.
Obai G, Odongo P & Wanyama R 2016. Prevalence of anaemia and associated risk factors among pregnant women attending antenatal care in Gulu and Hoima Regional Hospitals in Uganda: A cross sectional study. BMC pregnancy and childbirth. 16 (1): 1-7.
Padmanabhan A & Chandrakar S 2018. Autopsy study of maternal death in a tertiary care centre. Indian journal of obstetrics and gynecology. 5: 504-510.
Rai S 2018. Prevalence of anemia and associated factors among pregnant women od Itahari sub-Metropolitan city. DSpace repository: http:// 202. 45.146.37:8080/xmlui/handle/123456789/40.
Rasheed P, Koura MR, Al-Dabal BK & Makki SM 2008. Anemia in pregnancy: A study among attendees of primary health care centers. Annals of Saudi medicine. 28 (6): 449-452.
Stevens GA, et al. 2013. Global, regional, and national trends in haemoglobin concentration and prevalence of total and severe anaemia in children and pregnant and non-pregnant women for 1995–2011: a systematic analysis of population-representative data. Lancet global health. 1 (1): e16-e25.
Torheim LE, Ferguson EL, Penrose K & Arimond M 2010. Women in resource-poor settings are at risk of inadequate intakes of multiple micronutrients. Journal of nutrition. 140 (11): 2051S-2058S.
Webster-Gandy J, Madden A & Holdsworth M 2020. Oxford Handbook of Nutrition and Dietetics. Oxford University Press.
Willett W 1998. Reproducibility and validity of food-frequency questionnaires. Nutritional epidemiology. 101-147.
Zhang Q, Ananth CV, Rhoads GG & Li Z 2009. The impact of maternal anemia on perinatal mortality: a population-based, prospective cohort study in China. Annals of epidemiology. 19 (11): 793-799.
Conclusions
Findings showed that anemic females had higher tea consumption right after meals along with fewer intakes of protein, iron, and vitamin C as compared to the non-anemic females and RDA. Lack of education, lower literacy rate, less knowledge regarding balance diet, and improper iron supplementation among anemic females promoted higher prevalence of anemia in pregnancy.
Acknowledgments
We highly acknowledge the Preventive pediatrics department of Sir Ganga Ram Hospital, Lahore and Biostatistician (Ms. Humaira Waseem) of The University of Lahore for the guidance and cooperation.
Authors’ contributions
Humayun N conducted the study and collected the data. Bashir S supervised and designed the study, critical review of the manuscript and Khalid S literature search and manuscript write-up. All authors approved the final version of manuscript.
Conflict of interest
There is no conflict of interest to reveal.
Funding source
There was no funding source.
References
Abdelhafez AM & El-Soadaa SS 2012. Prevalence and risk factors of anemia among a sample of pregnant females attending primary health care centers in Makkah, Saudi Arabia. Pakistan journal of nutrition. 11 (12): 1113.
Alaofè H, Burney J, Naylor R & Taren D 2017. Prevalence of anaemia, deficiencies of iron and vitamin A and their determinants in rural women and young children: a cross-sectional study in Kalalé district of northern Benin. Public health nutrition. 20 (7): 1203-1213.
Alzaheb RA & Al-Amer O 2017. The prevalence of iron deficiency anemia and its associated risk factors among a sample of female university students in Tabuk, Saudi Arabia. Clinical medicine insights: women's health. 10: 1179562X17745088.
Aziz-Karim S, Khursheed M, Rizvi JH, Jafarey SN & Siddiqui RI 1990. Anaemia in pregnancy--a study of 709 women in Karachi. Tropical doctor. 20 (4): 184-185.
Baig-Ansari N, et al. 2008. Anemia prevalence and risk factors in pregnant women in an urban area of Pakistan. Food and nutrition bulletin. 29 (2): 132-139.
Balarajan Y, Ramakrishnan U, Özaltin E, Shankar AH & Subramanian S 2011. Anaemia in low-income and middle-income countries. lancet. 378 (9809): 2123-2135.
Bhutta Z, Soofi S, Zaidi S, Habib A & Hussain I 2011. National Nutrition Survey of Pakistan. Pakistan.
Kassebaum NJ 2016. The global burden of anemia. Hematology/Oncology clinics. 30 (2): 247-308.
Lone FW, Qureshi RN & Emanuel F 2004. Maternal anaemia and its impact on perinatal outcome. Tropical medicine & international health. 9 (4): 486-490.
Lozoff B, et al. 2006. Long-lasting neural and behavioral effects of iron deficiency in infancy. Nutrition reviews. 64 (suppl_2): S34-S43.
Nik Rosmawati N, Mohd Nazri S & Mohd Ismail I 2012. The rate and risk factors for anemia among pregnant mothers in Jerteh Terengganu, Malaysia. Journal of community medicine and health education. 2 (150): 2161-0711.
Obai G, Odongo P & Wanyama R 2016. Prevalence of anaemia and associated risk factors among pregnant women attending antenatal care in Gulu and Hoima Regional Hospitals in Uganda: A cross sectional study. BMC pregnancy and childbirth. 16 (1): 1-7.
Padmanabhan A & Chandrakar S 2018. Autopsy study of maternal death in a tertiary care centre. Indian journal of obstetrics and gynecology. 5: 504-510.
Rai S 2018. Prevalence of anemia and associated factors among pregnant women od Itahari sub-Metropolitan city. DSpace repository: http:// 202. 45.146.37:8080/xmlui/handle/123456789/40.
Rasheed P, Koura MR, Al-Dabal BK & Makki SM 2008. Anemia in pregnancy: A study among attendees of primary health care centers. Annals of Saudi medicine. 28 (6): 449-452.
Stevens GA, et al. 2013. Global, regional, and national trends in haemoglobin concentration and prevalence of total and severe anaemia in children and pregnant and non-pregnant women for 1995–2011: a systematic analysis of population-representative data. Lancet global health. 1 (1): e16-e25.
Torheim LE, Ferguson EL, Penrose K & Arimond M 2010. Women in resource-poor settings are at risk of inadequate intakes of multiple micronutrients. Journal of nutrition. 140 (11): 2051S-2058S.
Webster-Gandy J, Madden A & Holdsworth M 2020. Oxford Handbook of Nutrition and Dietetics. Oxford University Press.
Willett W 1998. Reproducibility and validity of food-frequency questionnaires. Nutritional epidemiology. 101-147.
Zhang Q, Ananth CV, Rhoads GG & Li Z 2009. The impact of maternal anemia on perinatal mortality: a population-based, prospective cohort study in China. Annals of epidemiology. 19 (11): 793-799.
Type of article: orginal article |
Subject:
public specific
Received: 2020/07/23 | Published: 2021/08/17 | ePublished: 2021/08/17
Received: 2020/07/23 | Published: 2021/08/17 | ePublished: 2021/08/17
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
