
Sat, Apr 27, 2024
[Archive]
Volume 2, Issue 2 (May 2017)
JNFS 2017, 2(2): 165-172 |
Back to browse issues page

Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Mozaffari-Khosravi H, Fallahi M, Afkhami-Ardekani M. Effect of Oral Supplementation of L-arginine on Sexual Function in Men with Type 2 Diabetes: A Double-blind Clinical Trial. JNFS 2017; 2 (2) :165-172
URL: http://jnfs.ssu.ac.ir/article-1-76-en.html
URL: http://jnfs.ssu.ac.ir/article-1-76-en.html


Department of Nutrition, School of Public Health, Shahid Sadoughi University of Medical Sciences, Yazd, Iran
Keywords: Arginine supplementation, Diabetes mellitus, Erectile dysfunction, Sexual dysfunction, Testosterone
Full-Text [PDF 431 kb]
(7804 Downloads)
| Abstract (HTML) (4524 Views)
Sexual dysfunction is common among diabetic men (Bacon et al., 2002, Enzlin et al., 2003, Thorve et al., 2011). The scientific associations consider the sexual health as the integrity and harmony between mind, emotions, and body, which makes growth of social and intellectual aspects and leads to make relationship and love. Any disorder that results in disharmony and thus lack of satisfaction in sex can cause sexual dysfunction (Rush and Blacker, 2008). ICD-10 criteria for sexual dysfunction are defined as:
The inability of a person to engage in sex
with biological or psychological origin. Erectile dysfunction (ED), one of the sexual dysfunction, is inability of getting and maintaining an erection for satisfactory sexual intercourse (World Health, 1996). Sexual dysfunction affects millions of men and their sexual partners' life quality in the world many of whom prefer to suffer in silence (Frank et al., 1978). The prevalence increased from 5% in people within the age range of 2024 to 50% in those from 55 to 59 years (Price, 2014).
It was estimated that in 2025 there will be around 322 million men who have experienced ED in the world and the largest increases will project in Africa, Asia, and South America, around 2.5 times more than the other areas (Aytac et al., 1999). The relationship between diabetes mellitus and the incidence of ED has been documented since 1798 and it was reported that generally 27-75% of men with type 2 diabetes (T2D) have experienced this problem (Bacon et al., 2002). In numerous epidemiological studies the odd ratio of having ED if a man is diabetic, is 1.9–4 times greater than a none diabetic population, making diabetes one of the greatest risk factors for ED (Lewis, 2001).
In addition, the causes of impotence can be divided into three group factors: (1) psychological issues, (2) physical issues, and (3) combination of both. Vascular disease and diabetes are the two main reasons lead to impotence with organic origin (Akhondzadeh et al., 2010). Different ways for impotence treatment are used, but to determine the effectiveness and side effects of these treatments other studies are needed.
L-arginine is an amino acid which is found in numerous foods. The effects of L-arginine supplementation have been investigated in some studies and the evidences were documented. One of the evidences is that L-arginine is the precursor of nitric oxide (NO), a neurotransmitters needed for relaxation of penis muscles (Lebret et al., 2002). L-arginine is an amino acid which is found in numerous foods. The effects of L-arginine supplementation have been investigated in some studies and the evidences were documented.
One of the evidences is that L-arginine is the precursor of nitric oxide (NO), a neurotransmitters needed for relaxation of penis muscles (Chen et al., 1999, Klotz et al., 1999, Moody et al., 1997, Ratnasooriya et al., 2000). Therefore, there is no consensus about the effects of L-arginine supplementation on sexual function, especially among T2D and further studies are needed. The objective of this study is to determine the effect of oral L-arginine supplementation on sexual function in men with T2D.
Materials and Methods
Study design and participants: This study is a double-blind controlled trial involving 80 patients with T2D selected from Yazd Diabetes Research Center (YDRC) in 2013-2014. YDRC is affiliated with Shahid Sadoughi University of Medical University and is an outpatient secondary referral center whose patients are referred by their primary health care practitioner. The general and specialty medical services provided to patients and research projects can also be performed in this center.
To calculate the sample size, it was considered
α = 0.05, power = 80%, mean and variance of sexual function score.(Chen et al., 1999) Also, with consideration of 10% drop out the result of
sample size will be 40 participants in each
group. Inclusion criteria included: being
married; patients with mild to moderate erectile dysfunction (according to the score 15 to 25 obtained from the questionnaire of international index of erectile function (IIEF)) (Mehraban et al., 2006); age between 25 to 55 years; a minimum of 5 years’ experience in diabetes. Exclusion criteria included: unstable cardiovascular status (angina and heart attack experience); cancer chemotherapy; use of medication for sexual activity; surgery
in the pelvic or prostate area; lack of personal satisfaction to log in to study; insulin users; consumers of opium and any apparent disorders of the genital system by endocrinologist assumption.
Patients were randomly assigned into 2 groups, L-arginine (AG) and placebo group (PG). Randomization was done via tables of random numbers which were then listed in sequential order. The allocation of patients and the subsequent follow-up was performed by secretaries. The AG took 5 g/day of L-arginine and the PG received the same amount of methyl cellulose for 4 weeks. To improve the taste, patients were advised to consume the powder dissolved in yogurt. Participants were masked during the treatment allocation because the taste and appearance of the yoghurt mixed L-arginine was identical to that of the PG. In order to follow the supplements taking, both groups were visited once a week and the residual and probably side effects were recorded.
Measurements: At the beginning of the intervention, some demographic variables of patients were recorded with interview. Weight was measured by digital scale with light clothing and accuracy of 0.1 kg and height was measured with accuracy of 0.5 cm without shoes. At the beginning and end of the study the questionnaire of IIEF was completed for each patient. This questionnaire was validated in Persian and it was used in many studies in Iran. The questionnaire was completed through interviews with patients by a general practitioner who was unaware of the participants' group. This questionnaire contained 15 questions and each question took a certain score. The total score determine sexual function: the total score of questions 1 to 5 and 15 indicate individual erectile function. Score lower than 15 indicates severe erectile dysfunction; scores in range of 15-25 show moderate erectile dysfunction; and scores more than 25 indicate no erectile dysfunction. In order to determine testosterone concentrations, 5 ml of blood samples were taken at the baseline and after the intervention. Samples were kept in -20 °C and testosterone was measured by radio immunoassay method at the end of intervention.
Ethical considerations: Written consent was obtained from participants at the beginning of the intervention. Entrance of the patients was completely voluntarily and all experiments
were free. This study was approved by the
Shahid Sadoughi University of Medical Sciences Research Ethic Committee. In addition, it
was registered in the Iranian Clinical Trial Registration Center (www.irct.ir) with the code
of IRCT2015050322076N1.
Data analysis: Data were analyzed through SPSS 21 Software. To specify the distribution of data, Kolmogrov Smirnov test was applied. Student t-test was used for comparing the mean of the quantitative variables between groups, and paired t-test was used for within group comparison. A p-value of < 0.05 was considered to be statistically significant.
Results
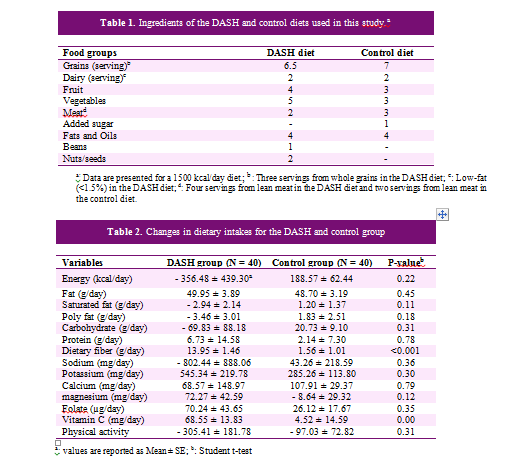
As it is shown in Figure 1, from AG 6 patients and from PG 5 patients were excluded and finally the data of 69 patients were analyzed. The means of demographic variables are reported in Table 1. There were no statistically significant differences in mean variables between the two groups.
Mean of sexual function parameters between and within groups are shown in Table 2. As it can be seen, the mean of total score and total changes of sexual function within AG, compared with PG, had significantly increased. Also, in contrast to PG, the means of all parameters were significantly improved in AG after intervention. The mean of “erectile function” within AG compared with PG had significantly increased. Mean of "sexual satisfaction" had significantly increased in AG, while there were no significant differences compared with PG. Changes in 'sexual desire' had results similar to 'sexual satisfaction'.
Table 3 shows means of testosterone concentration. As represented, the means of testosterone concentration significantly increased in both groups after the intervention, but its improvement was significantly higher in AG than PG (1.91 μg/L vs. 0.53 μg/L)
.
Discussion
This study showed that a daily intake of 5 g oral arginine supplementation for 4 weeks in men with T2D suffering from mild-to-moderate erectile dysfunction, has improved parameters like erectile function, sexual satisfaction, sexual desire, pleasure from sexual intercourse, and testosterone levels.
Improve erectile function in men may increase their confidence in sexual activities and thereby has a significant impact on improving their quality of life. Dadfar et al. explained that higher self confidence in men due to better erectile function, results in improvement of mentioned parameters (Dadfar et al., 2008), but there is still no adequate evidence and it needs further investigation. In a study conducted by Lebert et al., L-arginine and yohimbine were compared; results showed that arginine supplementation improved erectile function, while pure yohimbine supplementation did not have the same effect (Lebret et al., 2002). NO is a vasodilator that increases blood flow in penis arteries (Padma-Nathan, 2000). Arginine increases synthesis and release of NO, thus it can be the mechanism of arginine effect on erectile function.
Our study showed 5 g/day L-arginine for 4 weeks in T2D patients with mild-to-moderate erectile dysfunction improve concentration of total testosterone; Aoki et al. also showed the same result about oral L-arginine supplementation (Aoki et al., 2012). The exact mechanism of this increase is not clear yet. One of the mechanisms may be that arginine supplementation improves erectile function and thus increases confidence in sexual activities. Increase of self-confidence causes further sexual intercourse. This positive feedback increases the secretion of testosterone from the Leydig cells in the testes. On the other hand, arginine can increase the synthesis and release of NO and also increase blood flow to testes which lead to improve their performance in synthesis and secretion of testosterone (Lamm, 2009). Yasuda et al. in their study suggested that increased NO concentrations by increasing in cGMP release. cGMP is a vasodilator which increases blood flow in the testes as well as synthesis and secretion of testosterone in the Leydig cells (Yasuda et al., 2008).
It was recently reported that the reduction in hemodynamic parameters is a common condition between patients with T2D and leads to sexual dysfunctions and the other complications in patients through a reduction of NO mediated relaxation. There are also evidences that Phosphodiesterase-5 inhibitors have hemodynamic effects through the improving NO levels (Santi et al., 2015).
Small number of participants, short duration of the trial, and uncontrolled blood glucose during the intervention were the major limitation of our study. Further studies with longer period of time and more participants are needed. It is also recommended to control blood glucose during the intervention.
Conclusions
The present trial showed that daily consumption of 5g L-arginine for four weeks in T2D men with mild-to-moderate sexual dysfunction improves various parameters such as erectile function, sexual satisfaction, sexual desire, pleasure from sexual intercourse, marital satisfaction, and testosterone level.
Acknowledgments
We would like to thank Shahid Sadoughi University of Medical Sciences for funding this trial. Special thanks to the participants who participated in this study and the all staff of Yazd Diabetes Research Center.
Authors’ contributions
Mozaffari-Khosravi H participated to conception and design of study, managing the project and drafting the manuscript. Fallahi M and Afkhami-Ardekani M participated to acquisition of data, data analysis, selection of participants and drafting the manuscript. All authors read the paper and verified it.
Conflicts of interest
None declared.
Full-Text: (2011 Views)
Effect of Oral Supplementation of L-arginine on Sexual Function in Men with Type 2 Diabetes: A Double-blind Clinical Trial
Hassan Mozaffari-Khosravi; PhD1,2*, Mosayeb Fallahi; MSc1, Mohammad Afkhami-Ardekani; MD2,3
1 Department of Nutrition, School of Public Health, Shahid Sadoughi University of Medical Sciences, Yazd, Iran.
2 Yazd Diabetic Research Center, Shahid Sadoughi University of Medical Sciences, Yazd, Iran.
3 Department of Internal Medicine, School of Medicine, Shahid Sadoughi University of Medical Sciences, Yazd, Iran.
Hassan Mozaffari-Khosravi; PhD1,2*, Mosayeb Fallahi; MSc1, Mohammad Afkhami-Ardekani; MD2,3
1 Department of Nutrition, School of Public Health, Shahid Sadoughi University of Medical Sciences, Yazd, Iran.
2 Yazd Diabetic Research Center, Shahid Sadoughi University of Medical Sciences, Yazd, Iran.
3 Department of Internal Medicine, School of Medicine, Shahid Sadoughi University of Medical Sciences, Yazd, Iran.
| ARTICLE INFO | ABSTRACT | |
| ORIGINAL ARTICLE | Background: Sexual dysfunction is an important health problem which prevalence in patients with type 2 diabetes (T2D) is higher than other people. The aim of this study was to evaluate the effect of L-arginine oral supplementation on sexual function in men with T2D and mild-to-moderate erectile dysfunction (ED). Methods: Eighty men with T2D, suffering from mild-to-moderate erectile dysfunction participated in this double-blind clinical trial. They were randomly assigned in to two groups; receiving 5 g/day L-arginine (AG) or placebo group (PG) for 4 weeks. Sexual functions were recorded with international index of erectile function questionnaire at the beginning and end of the intervention. Total testosterone concentrations were measured too. Results: The total mean score of sexual function parameters significantly increased only in AG than PG (43.2 ± 6.2 vs. 39.4 ± 4.0, P = 0.003). Against PG, the mean of all parameters significantly improved in AG after intervention. Only the mean score of erectile function in AG had a significant increase compared to PG. Mean of other sexual activity scores between the two groups had no significant differences. The mean of testosterone concentration had a significant increase in both groups after the intervention, but the mean of changes was significantly higher in AG than in PG (1.91 μg/L vs. 0.53 μg/L, P = 0.004). Conclusions: The present trial showed that daily consumption of 5 g L-arginine for four weeks in T2D men with mild-to-moderate sexual dysfunction improved various parameters such as erectile function, sexual satisfaction, sexual desire, pleasure from sexual intercourse, and testosterone level. Keywords: Arginine supplementation; Diabetes mellitus; Erectile dysfunction; Sexual dysfunction; Testosterone |
|
| Article history: Received: 25 Dec 2016 Revised: 15 Jan 2017 Accepted: 12 Mar 2017 |
||
| IRCT code: 2015050322076N1 |
||
| *Corresponding author: mozaffari.kh@gmail.com Department of Nutrition, School of Public Health, Shahid Sadoughi University of Medical Sciences, Shohaday Gomname BLV, Yazd, Iran. Postal code: 8915173160 Tel: +98 35 38209143 |
Introduction
Sexual dysfunction is common among diabetic men (Bacon et al., 2002, Enzlin et al., 2003, Thorve et al., 2011). The scientific associations consider the sexual health as the integrity and harmony between mind, emotions, and body, which makes growth of social and intellectual aspects and leads to make relationship and love. Any disorder that results in disharmony and thus lack of satisfaction in sex can cause sexual dysfunction (Rush and Blacker, 2008). ICD-10 criteria for sexual dysfunction are defined as:
The inability of a person to engage in sex
with biological or psychological origin. Erectile dysfunction (ED), one of the sexual dysfunction, is inability of getting and maintaining an erection for satisfactory sexual intercourse (World Health, 1996). Sexual dysfunction affects millions of men and their sexual partners' life quality in the world many of whom prefer to suffer in silence (Frank et al., 1978). The prevalence increased from 5% in people within the age range of 2024 to 50% in those from 55 to 59 years (Price, 2014).
It was estimated that in 2025 there will be around 322 million men who have experienced ED in the world and the largest increases will project in Africa, Asia, and South America, around 2.5 times more than the other areas (Aytac et al., 1999). The relationship between diabetes mellitus and the incidence of ED has been documented since 1798 and it was reported that generally 27-75% of men with type 2 diabetes (T2D) have experienced this problem (Bacon et al., 2002). In numerous epidemiological studies the odd ratio of having ED if a man is diabetic, is 1.9–4 times greater than a none diabetic population, making diabetes one of the greatest risk factors for ED (Lewis, 2001).
In addition, the causes of impotence can be divided into three group factors: (1) psychological issues, (2) physical issues, and (3) combination of both. Vascular disease and diabetes are the two main reasons lead to impotence with organic origin (Akhondzadeh et al., 2010). Different ways for impotence treatment are used, but to determine the effectiveness and side effects of these treatments other studies are needed.
L-arginine is an amino acid which is found in numerous foods. The effects of L-arginine supplementation have been investigated in some studies and the evidences were documented. One of the evidences is that L-arginine is the precursor of nitric oxide (NO), a neurotransmitters needed for relaxation of penis muscles (Lebret et al., 2002). L-arginine is an amino acid which is found in numerous foods. The effects of L-arginine supplementation have been investigated in some studies and the evidences were documented.
One of the evidences is that L-arginine is the precursor of nitric oxide (NO), a neurotransmitters needed for relaxation of penis muscles (Chen et al., 1999, Klotz et al., 1999, Moody et al., 1997, Ratnasooriya et al., 2000). Therefore, there is no consensus about the effects of L-arginine supplementation on sexual function, especially among T2D and further studies are needed. The objective of this study is to determine the effect of oral L-arginine supplementation on sexual function in men with T2D.
Materials and Methods
Study design and participants: This study is a double-blind controlled trial involving 80 patients with T2D selected from Yazd Diabetes Research Center (YDRC) in 2013-2014. YDRC is affiliated with Shahid Sadoughi University of Medical University and is an outpatient secondary referral center whose patients are referred by their primary health care practitioner. The general and specialty medical services provided to patients and research projects can also be performed in this center.
To calculate the sample size, it was considered
α = 0.05, power = 80%, mean and variance of sexual function score.(Chen et al., 1999) Also, with consideration of 10% drop out the result of
sample size will be 40 participants in each
group. Inclusion criteria included: being
married; patients with mild to moderate erectile dysfunction (according to the score 15 to 25 obtained from the questionnaire of international index of erectile function (IIEF)) (Mehraban et al., 2006); age between 25 to 55 years; a minimum of 5 years’ experience in diabetes. Exclusion criteria included: unstable cardiovascular status (angina and heart attack experience); cancer chemotherapy; use of medication for sexual activity; surgery
in the pelvic or prostate area; lack of personal satisfaction to log in to study; insulin users; consumers of opium and any apparent disorders of the genital system by endocrinologist assumption.
Patients were randomly assigned into 2 groups, L-arginine (AG) and placebo group (PG). Randomization was done via tables of random numbers which were then listed in sequential order. The allocation of patients and the subsequent follow-up was performed by secretaries. The AG took 5 g/day of L-arginine and the PG received the same amount of methyl cellulose for 4 weeks. To improve the taste, patients were advised to consume the powder dissolved in yogurt. Participants were masked during the treatment allocation because the taste and appearance of the yoghurt mixed L-arginine was identical to that of the PG. In order to follow the supplements taking, both groups were visited once a week and the residual and probably side effects were recorded.
Measurements: At the beginning of the intervention, some demographic variables of patients were recorded with interview. Weight was measured by digital scale with light clothing and accuracy of 0.1 kg and height was measured with accuracy of 0.5 cm without shoes. At the beginning and end of the study the questionnaire of IIEF was completed for each patient. This questionnaire was validated in Persian and it was used in many studies in Iran. The questionnaire was completed through interviews with patients by a general practitioner who was unaware of the participants' group. This questionnaire contained 15 questions and each question took a certain score. The total score determine sexual function: the total score of questions 1 to 5 and 15 indicate individual erectile function. Score lower than 15 indicates severe erectile dysfunction; scores in range of 15-25 show moderate erectile dysfunction; and scores more than 25 indicate no erectile dysfunction. In order to determine testosterone concentrations, 5 ml of blood samples were taken at the baseline and after the intervention. Samples were kept in -20 °C and testosterone was measured by radio immunoassay method at the end of intervention.
Ethical considerations: Written consent was obtained from participants at the beginning of the intervention. Entrance of the patients was completely voluntarily and all experiments
were free. This study was approved by the
Shahid Sadoughi University of Medical Sciences Research Ethic Committee. In addition, it
was registered in the Iranian Clinical Trial Registration Center (www.irct.ir) with the code
of IRCT2015050322076N1.
Data analysis: Data were analyzed through SPSS 21 Software. To specify the distribution of data, Kolmogrov Smirnov test was applied. Student t-test was used for comparing the mean of the quantitative variables between groups, and paired t-test was used for within group comparison. A p-value of < 0.05 was considered to be statistically significant.
Results
As it is shown in Figure 1, from AG 6 patients and from PG 5 patients were excluded and finally the data of 69 patients were analyzed. The means of demographic variables are reported in Table 1. There were no statistically significant differences in mean variables between the two groups.
Mean of sexual function parameters between and within groups are shown in Table 2. As it can be seen, the mean of total score and total changes of sexual function within AG, compared with PG, had significantly increased. Also, in contrast to PG, the means of all parameters were significantly improved in AG after intervention. The mean of “erectile function” within AG compared with PG had significantly increased. Mean of "sexual satisfaction" had significantly increased in AG, while there were no significant differences compared with PG. Changes in 'sexual desire' had results similar to 'sexual satisfaction'.
Table 3 shows means of testosterone concentration. As represented, the means of testosterone concentration significantly increased in both groups after the intervention, but its improvement was significantly higher in AG than PG (1.91 μg/L vs. 0.53 μg/L)
.
| Table 1. Baseline characteristics | |||
| Characteristics | Arginine group (n = 34) | Placebo group (n = 35) | P-valuea |
| Age (y) | 51.58 ± 2.67 | 51.31 ± 2.65 | 0.99 |
| Duration of disease (y) | 10.58 ± 3.87 | 10.42 ± 4.17 | 0.83 |
| Height (cm) | 170.88 ± 7.57 | 171.40 ± 6.83 | 0.97 |
| Weight (kg) | 76.91 ± 11.69 | 78.17 ± 12.21 | 0.79 |
| BMI (kg/m2) | 26.29 ± 3.18 | 26.56 ± 3.68 | 0.14 |
| Waist circumference (cm) | 99.32 ± 8.05 | 99.88 ± 9.53 | 0.11 |
| Hip circumference (cm) | 94.94 ± 6.34 | 95.74 ± 5.96 | 0.45 |
a: Student t-test
| Table 2. Mean (±SD) and confidence interval 95% of sexual function parameters between and within groups | ||||||
| Sexual functions | Arginine group | Placebo group | P-valuea | |||
| Mean ± SD | CI 95% | Mean ± SD | CI 95% | |||
| Erectile function Before After |
16.32 ± 1.36 | 15.84-16.79 |
16.11 ± 1.30 | 15.66-16.56 |
0.51 |
|
| 18.67 ± 3.06 | 17.60-19.74 | 16.31 ± 1.92 | 15.65-16.97 | <0.001 | ||
| P-valueb | <0.001 | 0.485 | ||||
| Sexual satisfaction Before After |
5.08 ± 1.26 | 4.64-5.52 |
5.60 ± 1.06 | 5.23-5.96 |
0.07 |
|
| 5.58 ± 1.10 | 5.20-5.97 | 5.40 ± 1.06 | 5.03-5.76 | 0.47 | ||
| P-value | 0.004 | 0.090 | ||||
| Sexual desire Before After |
5.05 ± 0.91 | 4.03-5.37 |
5.37 ± 0.77 | 5.10-5.63 |
0.13 |
|
| 5.58 ± 0.98 | 5.24-5.93) | 5.22 ± 0.91 | 4.91-5.54 | 0.12 | ||
| P-value | 0.018 | 0.392 | ||||
| Pleasure from sexual intercourse Before After |
5.52 ± 1.46 |
5.01-6.03 |
6.22 ± 1.33 |
5.07-6.68 |
0.04 |
|
| 6.79 ± 1.66 | 6.21-7.37 | 6.25 ± 1.26 | 5.82-6.69 | 0.13 | ||
| P-value | <0.001 | 0.879 | ||||
| Marital satisfaction Before After |
6.64 ± 0.85 | 6.55-7.15 |
6.38 ± 0.75 | 6.03-6.54 |
0.15 |
|
| 6.85 ± 0.77 | 6.37-6.91 | 6.45 ± 0.75 | 5.90-6.61 | 0.81 | ||
| P-value | 0.33 | 0.83 | ||||
| Total score Before After |
38.8 ± 3.60 | 37.4-40.1 | 39.6 ± 3.09 | 38.5-40.2 | 0.35 | |
| 43.2 ± 6.02 | 41.1-45.3 | 39.4 ± 4.06 | 39.0-40.8 | 0.003 | ||
| P-value | <0.001 | 0.787. | ||||
| Total changes | 4.44 ± 5.7 | -0.14 ± 3.0 | <0.001 | |||
a: Student t-test; b Paired t-test, CI: Confidence interval 95%
| Table 3. Mean (± SD) and confidence interval 95% of testosterone concentration (μg/L) before and after intervention in both groups. | |||||
| P-valuea | Placebo group (n = 35) | Arginine group (n = 34) | Periods | ||
| CI 95% | Mean ± SD | CI 95% | Mean ± SD | ||
| 0.11 | 3.90-5.57 | 4.73 ± 2.42 | 3.67-4.96 | 4.32 ± 1.82 | Before |
| 0.82 | 4.52-6.01 | 5.27 ± 2.16 | 5.45-7.01 | 6.23 ± 2.23 | After |
| 0.004 | -0.14-1.23 | 0.53 ± 1.90 | 1.28-2.54 | 1.91 ± 1.80 | Changes |
| 0.001 | 0.001 | P-valueb | |||
a: Student t-test; b: Paired t-test, CI: Confidence interval 95%
Discussion
This study showed that a daily intake of 5 g oral arginine supplementation for 4 weeks in men with T2D suffering from mild-to-moderate erectile dysfunction, has improved parameters like erectile function, sexual satisfaction, sexual desire, pleasure from sexual intercourse, and testosterone levels.
Improve erectile function in men may increase their confidence in sexual activities and thereby has a significant impact on improving their quality of life. Dadfar et al. explained that higher self confidence in men due to better erectile function, results in improvement of mentioned parameters (Dadfar et al., 2008), but there is still no adequate evidence and it needs further investigation. In a study conducted by Lebert et al., L-arginine and yohimbine were compared; results showed that arginine supplementation improved erectile function, while pure yohimbine supplementation did not have the same effect (Lebret et al., 2002). NO is a vasodilator that increases blood flow in penis arteries (Padma-Nathan, 2000). Arginine increases synthesis and release of NO, thus it can be the mechanism of arginine effect on erectile function.
Our study showed 5 g/day L-arginine for 4 weeks in T2D patients with mild-to-moderate erectile dysfunction improve concentration of total testosterone; Aoki et al. also showed the same result about oral L-arginine supplementation (Aoki et al., 2012). The exact mechanism of this increase is not clear yet. One of the mechanisms may be that arginine supplementation improves erectile function and thus increases confidence in sexual activities. Increase of self-confidence causes further sexual intercourse. This positive feedback increases the secretion of testosterone from the Leydig cells in the testes. On the other hand, arginine can increase the synthesis and release of NO and also increase blood flow to testes which lead to improve their performance in synthesis and secretion of testosterone (Lamm, 2009). Yasuda et al. in their study suggested that increased NO concentrations by increasing in cGMP release. cGMP is a vasodilator which increases blood flow in the testes as well as synthesis and secretion of testosterone in the Leydig cells (Yasuda et al., 2008).
It was recently reported that the reduction in hemodynamic parameters is a common condition between patients with T2D and leads to sexual dysfunctions and the other complications in patients through a reduction of NO mediated relaxation. There are also evidences that Phosphodiesterase-5 inhibitors have hemodynamic effects through the improving NO levels (Santi et al., 2015).
Small number of participants, short duration of the trial, and uncontrolled blood glucose during the intervention were the major limitation of our study. Further studies with longer period of time and more participants are needed. It is also recommended to control blood glucose during the intervention.
Conclusions
The present trial showed that daily consumption of 5g L-arginine for four weeks in T2D men with mild-to-moderate sexual dysfunction improves various parameters such as erectile function, sexual satisfaction, sexual desire, pleasure from sexual intercourse, marital satisfaction, and testosterone level.
Acknowledgments
We would like to thank Shahid Sadoughi University of Medical Sciences for funding this trial. Special thanks to the participants who participated in this study and the all staff of Yazd Diabetes Research Center.
Authors’ contributions
Mozaffari-Khosravi H participated to conception and design of study, managing the project and drafting the manuscript. Fallahi M and Afkhami-Ardekani M participated to acquisition of data, data analysis, selection of participants and drafting the manuscript. All authors read the paper and verified it.
Conflicts of interest
None declared.
References
Akhondzadeh S, Amiri A & Bagheri AH 2010. Efficacy and Safety of Oral Combination of Yohimbine and L-arginine (SX) for the Treatment of Erectile Dysfunction: a multicenter, randomized, double blind, placebo-controlled clinical trial. Iranian journal of psychiatry. 5 (1): 1.
Aoki H, et al. 2012. Clinical Assessment of a Supplement of Pycnogenolآ® and L-arginine in Japanese Patients with Mild to Moderate Erectile Dysfunction. Phytotherapy research. 26 (2): 204-207.
Aytac IA, McKinlay JB & Krane RJ 1999. The likely worldwide increase in erectile dysfunction between 1995 and 2025 and some possible policy consequences. British journal urological international. 84: 50-56.
Bacon CG, et al. 2002. Association of type and duration of diabetes with erectile dysfunction in a large cohort of men. Diabetes care. 25 (8): 1458-1463.
Chen J, et al. 1999. Effect of oral administration of high-dose nitric oxide donor l-arginine in men with organic erectile dysfunction: results of a double-blind, randomized, placebo-controlled study. British journal urological international. 83: 269-273.
Dadfar M, Taei K & Ebrahimpur A 2008. A study on the effectiveness of atorvastatin in the treatment of erectile dysfunction in hypercholesterolemic men Jundishapur medical journal. 7 (1): 110-112.
Enzlin P, Mathieu C, Van den Bruel A, Vanderschueren D & Demyttenaere K 2003. Prevalence and predictors of sexual dysfunction in patients with type 1 diabetes. Diabetes care. 26 (2): 409-414.
Frank E, Anderson C & Rubinstein D 1978. Frequency of sexual dysfunction in normal couples. New England journal of medicine. 299 (3): 111-115.
Klotz T, Mathers MJ, Braun M, Bloch W & Engelmann U 1999. Effectiveness of oral L-arginine in first-line treatment of erectile dysfunction in a controlled crossover study. Urologia internationalis. 63 (4): 220-223.
Lamm S 2009. Preloxآ® for improvement of erectile quality. European journal of endocrinology. 5: 70-74.
Lebret T, Hervأ© J-M, Gorny P, Worcel M & Botto H 2002. Efficacy and safety of a novel combination of L-arginine glutamate and yohimbine hydrochloride: a new oral therapy for erectile dysfunction. European urology. 41 (6): 608-613.
Lewis RW 2001. Epidemiology of erectile dysfunction. Urologic clinics of north America. 28 (2): 209-216.
Mehraban D, Shabaninia SH, Naderi GH & Esfahani F 2006. Farsi international index of erectile dysfunction and doppler ultrasonography in the evaluation of male impotence. Iranian journal of surgery. 14 (1): 25-31.
Moody JA, Vernet D, Laidlaw S, Rajfer J & Gonzalez-Cadavid NF 1997. Effects of long-term oral administration of L-arginine on the rat erectile response. The journal of urology. 158 (3): 942-947.
Padma-Nathan H 2000. Hemodynamic effects of the oral administration of a combination of Arginine and Yohimbine measured by Color Duplex Ultrasonography in men with Erectile Dysfunction. In annual meeting of the European society for impotence research, poster.
Price D 2014. Sexual problems in diabetes. Medicine. 43 (1): 38-40.
Ratnasooriya WD, Dharmasiri MG & Wadsworth RM 2000. Reduction in libido and fertility of male rats by administration of the nitric oxide (NO) synthase inhibitor N-nitro-l-arginine methyl ester. International journal of andrology. 23 (3): 187-191.
Rush AJ & Blacker D 2008. Handbook of psychiatric measures. American Psychiatric Pub.
Santi D, et al. 2015. Therapy of endocrine disease. Effects of chronic use of phosphodiesterase inhibitors on endothelial markers in type 2 diabetes mellitus: a meta-analysis. European journal of endocrinology. 172 (3): R103-114.
Thorve VS, et al. 2011. Diabetes-induced erectile dysfunction: epidemiology, pathophysiology and management. Journal of diabetes and its complications. 25 (2): 129-136.
World Health O 1996. Multiaxial classification of child and adolescent psychiatric disorders: the ICD-10 classification of mental and behavioural disorders in children and adolescents. Cambridge University Press.
Yasuda M, et al. 2008. Salivary 8-OHdG: A Useful Biomarker for Predicting Severe ED and Hypogonadism. The journal of sexual medicine. 5 (6): 1482-1491.
Aoki H, et al. 2012. Clinical Assessment of a Supplement of Pycnogenolآ® and L-arginine in Japanese Patients with Mild to Moderate Erectile Dysfunction. Phytotherapy research. 26 (2): 204-207.
Aytac IA, McKinlay JB & Krane RJ 1999. The likely worldwide increase in erectile dysfunction between 1995 and 2025 and some possible policy consequences. British journal urological international. 84: 50-56.
Bacon CG, et al. 2002. Association of type and duration of diabetes with erectile dysfunction in a large cohort of men. Diabetes care. 25 (8): 1458-1463.
Chen J, et al. 1999. Effect of oral administration of high-dose nitric oxide donor l-arginine in men with organic erectile dysfunction: results of a double-blind, randomized, placebo-controlled study. British journal urological international. 83: 269-273.
Dadfar M, Taei K & Ebrahimpur A 2008. A study on the effectiveness of atorvastatin in the treatment of erectile dysfunction in hypercholesterolemic men Jundishapur medical journal. 7 (1): 110-112.
Enzlin P, Mathieu C, Van den Bruel A, Vanderschueren D & Demyttenaere K 2003. Prevalence and predictors of sexual dysfunction in patients with type 1 diabetes. Diabetes care. 26 (2): 409-414.
Frank E, Anderson C & Rubinstein D 1978. Frequency of sexual dysfunction in normal couples. New England journal of medicine. 299 (3): 111-115.
Klotz T, Mathers MJ, Braun M, Bloch W & Engelmann U 1999. Effectiveness of oral L-arginine in first-line treatment of erectile dysfunction in a controlled crossover study. Urologia internationalis. 63 (4): 220-223.
Lamm S 2009. Preloxآ® for improvement of erectile quality. European journal of endocrinology. 5: 70-74.
Lebret T, Hervأ© J-M, Gorny P, Worcel M & Botto H 2002. Efficacy and safety of a novel combination of L-arginine glutamate and yohimbine hydrochloride: a new oral therapy for erectile dysfunction. European urology. 41 (6): 608-613.
Lewis RW 2001. Epidemiology of erectile dysfunction. Urologic clinics of north America. 28 (2): 209-216.
Mehraban D, Shabaninia SH, Naderi GH & Esfahani F 2006. Farsi international index of erectile dysfunction and doppler ultrasonography in the evaluation of male impotence. Iranian journal of surgery. 14 (1): 25-31.
Moody JA, Vernet D, Laidlaw S, Rajfer J & Gonzalez-Cadavid NF 1997. Effects of long-term oral administration of L-arginine on the rat erectile response. The journal of urology. 158 (3): 942-947.
Padma-Nathan H 2000. Hemodynamic effects of the oral administration of a combination of Arginine and Yohimbine measured by Color Duplex Ultrasonography in men with Erectile Dysfunction. In annual meeting of the European society for impotence research, poster.
Price D 2014. Sexual problems in diabetes. Medicine. 43 (1): 38-40.
Ratnasooriya WD, Dharmasiri MG & Wadsworth RM 2000. Reduction in libido and fertility of male rats by administration of the nitric oxide (NO) synthase inhibitor N-nitro-l-arginine methyl ester. International journal of andrology. 23 (3): 187-191.
Rush AJ & Blacker D 2008. Handbook of psychiatric measures. American Psychiatric Pub.
Santi D, et al. 2015. Therapy of endocrine disease. Effects of chronic use of phosphodiesterase inhibitors on endothelial markers in type 2 diabetes mellitus: a meta-analysis. European journal of endocrinology. 172 (3): R103-114.
Thorve VS, et al. 2011. Diabetes-induced erectile dysfunction: epidemiology, pathophysiology and management. Journal of diabetes and its complications. 25 (2): 129-136.
World Health O 1996. Multiaxial classification of child and adolescent psychiatric disorders: the ICD-10 classification of mental and behavioural disorders in children and adolescents. Cambridge University Press.
Yasuda M, et al. 2008. Salivary 8-OHdG: A Useful Biomarker for Predicting Severe ED and Hypogonadism. The journal of sexual medicine. 5 (6): 1482-1491.
Type of article: orginal article |
Subject:
public specific
Received: 2016/10/24 | Published: 2017/05/1 | ePublished: 2017/05/1
Received: 2016/10/24 | Published: 2017/05/1 | ePublished: 2017/05/1
References
1. Efficacy and Safety of Oral Combination of Yohimbine and L-arginine (SX) for the Treatment of Erectile Dysfunction: a multicenter, randomized, double blind, placebo-controlled clinical trial. Iranian journal of psychiatry. 5 (1): 1.
2. Aoki H, et al. 2012. Clinical Assessment of a Supplement of Pycnogenolآ® and L-arginine in Japanese Patients with Mild to Moderate Erectile Dysfunction. Phytotherapy research. 26 (2): 204-207.
3. Aytac IA, McKinlay JB & Krane RJ 1999. The likely worldwide increase in erectile dysfunction between 1995 and 2025 and some possible policy consequences. British journal urological international. 84: 50-56.
4. Bacon CG, et al. 2002. Association of type and duration of diabetes with erectile dysfunction in a large cohort of men. Diabetes care. 25 (8): 1458-1463.
5. Chen J, et al. 1999. Effect of oral administration of high-dose nitric oxide donor l-arginine in men with organic erectile dysfunction: results of a double-blind, randomized, placebo-controlled study. British journal urological international. 83: 269-273.
6. Dadfar M, Taei K & Ebrahimpur A 2008. A study on the effectiveness of atorvastatin in the treatment of erectile dysfunction in hypercholesterolemic men Jundishapur medical journal. 7 (1): 110-112.
7. Enzlin P, Mathieu C, Van den Bruel A, Vanderschueren D & Demyttenaere K 2003. Prevalence and predictors of sexual dysfunction in patients with type 1 diabetes. Diabetes care. 26 (2): 409-414.
8. Frank E, Anderson C & Rubinstein D 1978. Frequency of sexual dysfunction in normal couples. New England journal of medicine. 299 (3): 111-115.
9. Klotz T, Mathers MJ, Braun M, Bloch W & Engelmann U 1999. Effectiveness of oral L-arginine in first-line treatment of erectile dysfunction in a controlled crossover study. Urologia internationalis. 63 (4): 220-223.
10. Lamm S 2009. Preloxآ® for improvement of erectile quality. European journal of endocrinology. 5: 70-74.
11. Lebret T, Hervأ© J-M, Gorny P, Worcel M & Botto H 2002. Efficacy and safety of a novel combination of L-arginine glutamate and yohimbine hydrochloride: a new oral therapy for erectile dysfunction. European urology. 41 (6): 608-613.
12. Lewis RW 2001. Epidemiology of erectile dysfunction. Urologic clinics of north America. 28 (2): 209-216.
13. Mehraban D, Shabaninia SH, Naderi GH & Esfahani F 2006. Farsi international index of erectile dysfunction and doppler ultrasonography in the evaluation of male impotence. Iranian journal of surgery. 14 (1): 25-31.
14. Moody JA, Vernet D, Laidlaw S, Rajfer J & Gonzalez-Cadavid NF 1997. Effects of long-term oral administration of L-arginine on the rat erectile response. The journal of urology. 158 (3): 942-947.
15. Padma-Nathan H 2000. Hemodynamic effects of the oral administration of a combination of Arginine and Yohimbine measured by Color Duplex Ultrasonography in men with Erectile Dysfunction. In annual meeting of the European society for impotence research, poster.
16. Price D 2014. Sexual problems in diabetes. Medicine. 43 (1): 38-40.
17. Ratnasooriya WD, Dharmasiri MG & Wadsworth RM 2000. Reduction in libido and fertility of male rats by administration of the nitric oxide (NO) synthase inhibitor N-nitro-l-arginine methyl ester. International journal of andrology. 23 (3): 187-191.
18. Rush AJ & Blacker D 2008. Handbook of psychiatric measures. American Psychiatric Pub.
19. Santi D, et al. 2015. Therapy of endocrine disease. Effects of chronic use of phosphodiesterase inhibitors on endothelial markers in type 2 diabetes mellitus: a meta-analysis. European journal of endocrinology. 172 (3): R103-114.
20. Thorve VS, et al. 2011. Diabetes-induced erectile dysfunction: epidemiology, pathophysiology and management. Journal of diabetes and its complications. 25 (2): 129-136.
21. World Health O 1996. Multiaxial classification of child and adolescent psychiatric disorders: the ICD-10 classification of mental and behavioural disorders in children and adolescents. Cambridge University Press.
22. Yasuda M, et al. 2008. Salivary 8-OHdG: A Useful Biomarker for Predicting Severe ED and Hypogonadism. The journal of sexual medicine. 5 (6): 1482-1491.
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
