
Sat, May 4, 2024
[Archive]
Volume 5, Issue 1 (Feb 2020)
JNFS 2020, 5(1): 66-75 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Hasanizadeh S, Nadjarzadeh A, Mirzaei M, Salehi-Abargouei A, Hosseinzadeh M. The Association between Macronutrient Intake and the Metabolic Syndrome in Yazdian Adult Population. JNFS 2020; 5 (1) :66-75
URL: http://jnfs.ssu.ac.ir/article-1-293-en.html
URL: http://jnfs.ssu.ac.ir/article-1-293-en.html
Shirin Hasanizadeh 

 , Azadeh Nadjarzadeh , Masoud Mirzaei , Amin Salehi-Abargouei , Mahdieh Hosseinzadeh *
, Azadeh Nadjarzadeh , Masoud Mirzaei , Amin Salehi-Abargouei , Mahdieh Hosseinzadeh *
, Azadeh Nadjarzadeh , Masoud Mirzaei , Amin Salehi-Abargouei , Mahdieh Hosseinzadeh *
Department of Nutrition, School of Public Health, Shahid Sadoughi University of Medical Sciences, Yazd, Iran
Full-Text [PDF 527 kb]
(603 Downloads)
| Abstract (HTML) (2395 Views)
Full-Text: (577 Views)
The Association between Macronutrient Intake and the Metabolic Syndrome in Yazdian Adult Population
Shirin Hasanizadeh; MSc1,2, Azadeh Nadjarzadeh; PhD 1,2, Masoud Mirzaei; MD-PhD 3,
Amin Salehi-Abargouei; PhD 1.2 & Mahdieh Hosseinzadeh; PhD *1.2
1 Department of Nutrition, School of Public Health, Shahid Sadoughi University of Medical Sciences, Yazd, Iran.
2 Nutrition and Food Security Research Center, Shahid Sadoughi University of Medical Sciences, Yazd, Iran.
3 Yazd Cardiovascular Research Centre, Shahid Sadoughi University of Medical Sciences, Yazd-Iran.
Amin Salehi-Abargouei; PhD 1.2 & Mahdieh Hosseinzadeh; PhD *1.2
1 Department of Nutrition, School of Public Health, Shahid Sadoughi University of Medical Sciences, Yazd, Iran.
2 Nutrition and Food Security Research Center, Shahid Sadoughi University of Medical Sciences, Yazd, Iran.
3 Yazd Cardiovascular Research Centre, Shahid Sadoughi University of Medical Sciences, Yazd-Iran.
| ARTICLE INFO | ABSTRACT | |
| ORIGINAL ARTICLE | Background: Metabolic syndrome (MetS) is a collection of metabolic disorders including abdominal obesity, dyslipidemia, high glucose levels, and high blood pressure. The macronutrients such as carbohydrates, proteins, and fats are the effective factors in the occurrence of MetS. This study aimed to determine the association between the macronutrients intake and MetS in 20-69 year-old adult population of Yazd Greater Area, Iran. Methods: This study used Yazd Health Study (YaHS) recruitment phase data. The YaHS was a prospective cohort conducted on a random sample of 10,000 Yazdian adults aged 20-69 years. To conduct this study data from TaMeZ (Taghzieh Mardom-e-Yazd) or Yazd Nutrition Study, which was a nutrition study associated with YaHS were also used. MetS was defined according to the ATP III criteria. Dietary intake was evaluated using Food Frequency Questionnaire (FFQ). To evaluate the relationship between macronutrients and MetS, multivariate logistic regression analysis was used. Results: The odds ratio for the incidence of MetS was significantly higher in individuals who consumed higher amounts of carbohydrates. However, fat and protein intake did not have any significant relationship with odds of the developing MetS. Individuals with higher intake of carbohydrates had significantly higher odds of abdominal obesity (OR: 1.89, CI: 1.06-3.34); whereas, the probability of abdominal obesity decreased significantly in the highest quintile of protein intake (OR: 0.45, CI: 0.25-0.79). Conclusion: High intakes of carbohydrate increased the odds of getting to MetS and abdominal obesity. However, high levels of protein reduced the odds of abdominal obesity. No association was found between fat intake and the odds of the MetS. More prospective studies are needed to determine the role of macronutrients in MetS. Keywords: Metabolic syndrome (MetS); Macronutrien;, Carbohydrate; Protein; Fat |
|
| Article history: Received: 25 Aug 2019 Revised: 3 Nov 2019 Accepted: 17 Dec 2019 |
||
| *Corresponding author: hoseinzade.mahdie@gmail.com Department of Nutrition, School of Public Health, Shahid Sadoughi University of Medical Sciences, Yazd, Iran. Postal code: 8915173160 Tel: +98 35 38209100-14 |
Introduction
Metabolic syndrome (MetS) is a combination of metabolic disorders such as abdominal obesity, dyslipidemia, high glucose levels, and high blood pressure (Linardakis et al., 2008). These factors increase the risk of cardiovascular disease, arthritis, chronic kidney disease, and type 2 diabetes directly and indirectly (Lakka et al., 2002). The high prevalence of MetS in developed and developing countries has been investigated by many researchers (Kolovou et al., 2007). MetS has an incidence rate of about 34 and 35 percent among the adults of US (Esposito and Giugliano, 2010) and Iran (Delavari et al., 2009), respectively. In addition, MetS is more prevalent among the Iranian women than other women in the world (Dalvand et al., 2017).
Metabolic syndrome (MetS) is a combination of metabolic disorders such as abdominal obesity, dyslipidemia, high glucose levels, and high blood pressure (Linardakis et al., 2008). These factors increase the risk of cardiovascular disease, arthritis, chronic kidney disease, and type 2 diabetes directly and indirectly (Lakka et al., 2002). The high prevalence of MetS in developed and developing countries has been investigated by many researchers (Kolovou et al., 2007). MetS has an incidence rate of about 34 and 35 percent among the adults of US (Esposito and Giugliano, 2010) and Iran (Delavari et al., 2009), respectively. In addition, MetS is more prevalent among the Iranian women than other women in the world (Dalvand et al., 2017).
Among various factors including race, family history of chronic diseases, age, and gender, diet plays an important role in the development and control of MetS and its components (Kaur, 2014, Povel et al., 2012). No specific diet has been introduced to treat MetS. Some studies have shown the beneficial effects of Mediterranean (Esposito and Giugliano, 2010) and DASH diets (Azadbakht et al., 2005) on improving components of the MetS. Consumption of some nutrients and food groups (Casas-Agustench et al., 2011, Esmaillzadeh et al., 2005) was also reported to reduce the risk factors of this syndrome. In recent years, the combination of macronutrients in the diet of patients with MetS has attracted extensive attention. Since fats have the highest energy density among macronutrients, dietitians recommend individuals to reduce its consumption (Johnson et al., 2007). However, we should note that a reduction in the percentage of calorie received from the fats is associated with increased calorie intake from carbohydrates. High intake of carbohydrate increases serum triglycerides, decreases serum HDL-C, and impairs glucose metabolism as components of the MetS (McKeown et al., 2004, Mittendorfer and Sidossis, 2001). Considering the effect of consuming macronutrients such as lipids, proteins, and carbohydrates on the MetS, the findings of different studies are inconsistent (Carnethon et al., 2004).
For example, a cross-sectional study on Framingham research found no significant relationship between carbohydrate intake and MetS (McKeown et al., 2004). Similarly, the results of another study on men and women did not show any association between macronutrients' intake and MetS (Eilat-Adar et al., 2008). However, the results of a cross-sectional study on 1626 patients with history of cardiovascular diseases showed that high consumption of carbohydrates decreased the prevalence of MetS (Skilton et al., 2008). Furthermore, the results of a prospective study in this area indicated that high intake of fat was associated with increased risk of MetS (Skilton et al., 2008).
In this area, the results are controversial and the distribution of macronutrients in diets can determine the successful prevention and treatment of MetS. Moreover, no recommendation has ever been made to set up an appropriate diet for treatment of MetS. So, the current study was conducted to evaluate the effect of macronutrients on MetS and its components in adult population of Yazd city.
Materials and Methods
Participants and design: This cross-sectional study was carried on the data collected by two prospective studies; Yazd Health Study (YaHS ) and TAghzieh Mardom-e-YaZd (TAMEZ) or Yazd Nutrition Study. The study population included people who lived in Yazd city and were in the age range of 20-69 years. The study design, sampling method, participants' characteristics, and data collection method were published elsewhere (Mirzaei et al., 2017).
Initially, we studied the data of TAMEZ and YaHS to extract the required information on participants' dietary intake, anthropometric indices measurement, blood factors, blood pressure measurement, and confounding factors including socioeconomic status, history of chronic diseases, and physical activity status. Later, we merged the data of the above mentioned research projects.
Finally, of 3826 available profiles, 383 were excluded due to lack of specific codes (n = 2), lack of nutrition information (n = 332), repeated codes (n = 49), and lack of information on metabolic syndrome (n = 105). Finally, 3338 participants entered the study. In the next stage, we excluded people with a history of cardiovascular disease, stroke, diabetes, and cancer as well as individuals with higher or lower energy intakes (more than 6500 kcal and less than 600 kcal, respectively). Finally, the analysis was conducted on 2221 individuals.
Diet evaluation: Participants' dietary information was collected by completing a semi-quantitative FFQ consisting of 178 food items and 551 questions. The validity and reliability of this questionnaire was measured and confirmed in TAMEZ project (Mirzaei et al., 2017). In order to complete this questionnaire, we explained the average size of each food item for the participants and asked them to report the amount and frequency of that food. Later, the values related to each food item were determined in grams using guidelines of household scales (Ghaffarpour et al., 1999). The amount of energy, protein, carbohydrate, and fat intake was also determined.
Diagnosis of MetS: MetS was diagnosed in accordance with National cholesterol education program adult panel III (ATP III) (Alberti et al., 2009). Accordingly, the MetS was defined as having at least 3 cases of metabolic sub-syndrome factors: 1) Triglyceride above 150 mg/dl; 2) HDL cholesterol level of less than 40 mg/dl in men and less than 50 mg/dl in women; 3) Systolic blood pressure above 130 mmHg and diastolic blood pressure above 850 mmHg; 4) Fasting blood glucose above 110 mg/dl; and 5) waist circumference (WC) above 102 cm in men and 88 cm in women.
Evaluation of anthropometric indices: The participants' weights were measured using a digital scale (Omron BF511 Inc. Nagoya, Japan) with an accuracy of 0.1 kg. The height was also measured in standing position using the tape meter with an accuracy of 0.1 cm while the participants were leaning against a smooth wall without shoes. Waist circumference was measured with an accuracy of 0.5 cm using a tape measure in the horizontal plane midway between the lowest ribs and the iliac crest. The hip circumference was also measured at the largest part of the hips with an accuracy of 0.5 cm. All measurements were performed three times (before the interview, after completing one third of the questionnaire, after completing two third of the questionnaire). Later, we calculated the body mass index (BMI) by dividing the weight in kilograms by height in meters squared.
Blood pressure measurement: Systolic and diastolic blood pressures were measured in the sitting position after completing two-thirds of the questionnaire, which was after about 40 minutes of rest. The measurements were repeated three times with five-minute intervals using the Richter pressure gauge. Next, average of the second and the third measures was calculated and recorded as the blood pressure.
Laboratory data: Later, we measured the fasting blood glucose (FBG) (mg/dl), high density lipoprotein-cholesterol (HDL-C), and triglycerides (TG). An auto-analyzer device and kits related to each test (Pars Azmoon) were used for this purpose.
Other variables: Physical activity information was collected using a standard questionnaire (Mirzaei et al., 2017). Then, the amount of physical activity was calculated in metabolic equivalent of an hour per week. Furthermore, the participants' socioeconomic status and smoking status were collected using questionnaires and interviews (Mirzaei et al., 2017).
Data analysis: In order to carry out the analyses, we used the IBM SPSS version 22. For quantitative variables, the values were reported in mean and standard deviations and percentages were applied to report the classified variables. Student t-test and chi-square tests were also used to compare the quantitative and qualitative variables, respectively. The intake of macronutrients (grams per day) was adjusted based on the total energy intake and participants were divided into quantiles according to their consumption of macronutrients. These quantiles were then used as qualitative variables in the next statistical analyses. Finally, to evaluate the association of macronutrients' intake with the risk of metabolic syndrome and its components, we run multivariate regression after adjusting for the confounding variables such as age, education, gender, physical activity, smoking status, BMI, and family history of Chronic diseases.
Ethical considerations: both YaHS and TAMEZ studies have ethical approval from the Ethics Committee of Shahid Sadoughi University of Medical Sciences. Informed consents were also obtained from all participants.
Results
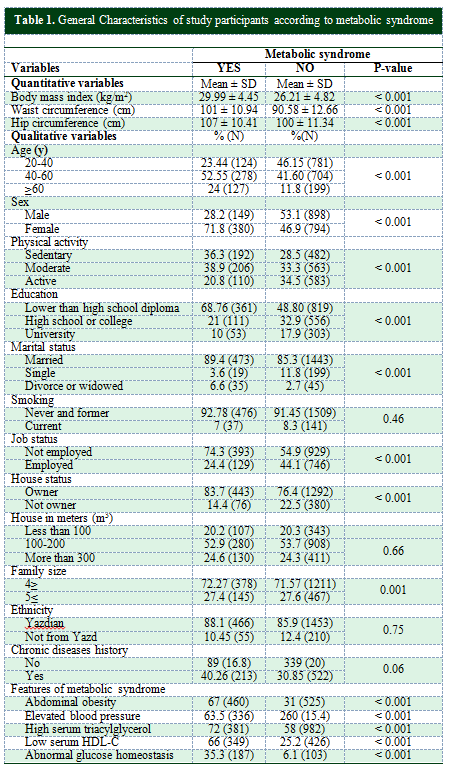
A cross-sectional study was carried out on 2221 individuals; 529 were afflicted with the MetS and 1692 did not have it. The general characteristics of the study participants are shown in Table 1. The BMI, WC, hip circumference, blood pressure, TG, and FBG were significantly higher in people with MetS. Moreover, 71 percent of the individual with MetS were women over 40 years of age.
A significant difference was observed between individuals with and without metabolic syndrome in terms of physical activity, education, marital status, occupational status, home ownership, and the number of family members. However, no significant difference was observed between the two groups regarding smoking status, ethnicity, house in meters, and the history of chronic diseases.
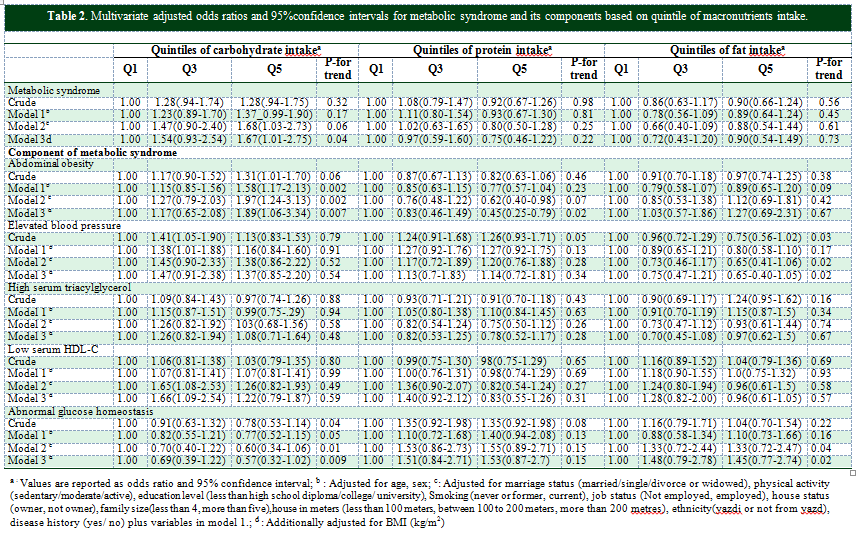
Table 2 shows the odds ratio of MetS and 95 percent confidence interval for intake of macronutrients in the crude model and after adjusting for the confounding factors in three models.
We adjusted for the confounding variables such as age, education, gender, physical activity, smoking status, BMI, and family history of chronic diseases and found that the odds ratio of MetS was significantly higher in individuals with more intake of carbohydrates (OR: 1.67, CI: 1.01-2.75). However, intake of fat and protein did not have any significant association with the probability of developing MetS (OR: 0.97, CI: 0.59-1.60, OR: 0.90, CI: 0.54-1.49).
Furthermore, individuals with higher intake of carbohydrates had more probability of abdominal obesity (OR: 1.89, CI: 1.06-3.34); whereas, higher consumption of proteins reduced the probability of abdominal obesity (OR: 0.45, CI: 0.25-0.79).
For example, a cross-sectional study on Framingham research found no significant relationship between carbohydrate intake and MetS (McKeown et al., 2004). Similarly, the results of another study on men and women did not show any association between macronutrients' intake and MetS (Eilat-Adar et al., 2008). However, the results of a cross-sectional study on 1626 patients with history of cardiovascular diseases showed that high consumption of carbohydrates decreased the prevalence of MetS (Skilton et al., 2008). Furthermore, the results of a prospective study in this area indicated that high intake of fat was associated with increased risk of MetS (Skilton et al., 2008).
In this area, the results are controversial and the distribution of macronutrients in diets can determine the successful prevention and treatment of MetS. Moreover, no recommendation has ever been made to set up an appropriate diet for treatment of MetS. So, the current study was conducted to evaluate the effect of macronutrients on MetS and its components in adult population of Yazd city.
Materials and Methods
Participants and design: This cross-sectional study was carried on the data collected by two prospective studies; Yazd Health Study (YaHS ) and TAghzieh Mardom-e-YaZd (TAMEZ) or Yazd Nutrition Study. The study population included people who lived in Yazd city and were in the age range of 20-69 years. The study design, sampling method, participants' characteristics, and data collection method were published elsewhere (Mirzaei et al., 2017).
Initially, we studied the data of TAMEZ and YaHS to extract the required information on participants' dietary intake, anthropometric indices measurement, blood factors, blood pressure measurement, and confounding factors including socioeconomic status, history of chronic diseases, and physical activity status. Later, we merged the data of the above mentioned research projects.
Finally, of 3826 available profiles, 383 were excluded due to lack of specific codes (n = 2), lack of nutrition information (n = 332), repeated codes (n = 49), and lack of information on metabolic syndrome (n = 105). Finally, 3338 participants entered the study. In the next stage, we excluded people with a history of cardiovascular disease, stroke, diabetes, and cancer as well as individuals with higher or lower energy intakes (more than 6500 kcal and less than 600 kcal, respectively). Finally, the analysis was conducted on 2221 individuals.
Diet evaluation: Participants' dietary information was collected by completing a semi-quantitative FFQ consisting of 178 food items and 551 questions. The validity and reliability of this questionnaire was measured and confirmed in TAMEZ project (Mirzaei et al., 2017). In order to complete this questionnaire, we explained the average size of each food item for the participants and asked them to report the amount and frequency of that food. Later, the values related to each food item were determined in grams using guidelines of household scales (Ghaffarpour et al., 1999). The amount of energy, protein, carbohydrate, and fat intake was also determined.
Diagnosis of MetS: MetS was diagnosed in accordance with National cholesterol education program adult panel III (ATP III) (Alberti et al., 2009). Accordingly, the MetS was defined as having at least 3 cases of metabolic sub-syndrome factors: 1) Triglyceride above 150 mg/dl; 2) HDL cholesterol level of less than 40 mg/dl in men and less than 50 mg/dl in women; 3) Systolic blood pressure above 130 mmHg and diastolic blood pressure above 850 mmHg; 4) Fasting blood glucose above 110 mg/dl; and 5) waist circumference (WC) above 102 cm in men and 88 cm in women.
Evaluation of anthropometric indices: The participants' weights were measured using a digital scale (Omron BF511 Inc. Nagoya, Japan) with an accuracy of 0.1 kg. The height was also measured in standing position using the tape meter with an accuracy of 0.1 cm while the participants were leaning against a smooth wall without shoes. Waist circumference was measured with an accuracy of 0.5 cm using a tape measure in the horizontal plane midway between the lowest ribs and the iliac crest. The hip circumference was also measured at the largest part of the hips with an accuracy of 0.5 cm. All measurements were performed three times (before the interview, after completing one third of the questionnaire, after completing two third of the questionnaire). Later, we calculated the body mass index (BMI) by dividing the weight in kilograms by height in meters squared.
Blood pressure measurement: Systolic and diastolic blood pressures were measured in the sitting position after completing two-thirds of the questionnaire, which was after about 40 minutes of rest. The measurements were repeated three times with five-minute intervals using the Richter pressure gauge. Next, average of the second and the third measures was calculated and recorded as the blood pressure.
Laboratory data: Later, we measured the fasting blood glucose (FBG) (mg/dl), high density lipoprotein-cholesterol (HDL-C), and triglycerides (TG). An auto-analyzer device and kits related to each test (Pars Azmoon) were used for this purpose.
Other variables: Physical activity information was collected using a standard questionnaire (Mirzaei et al., 2017). Then, the amount of physical activity was calculated in metabolic equivalent of an hour per week. Furthermore, the participants' socioeconomic status and smoking status were collected using questionnaires and interviews (Mirzaei et al., 2017).
Data analysis: In order to carry out the analyses, we used the IBM SPSS version 22. For quantitative variables, the values were reported in mean and standard deviations and percentages were applied to report the classified variables. Student t-test and chi-square tests were also used to compare the quantitative and qualitative variables, respectively. The intake of macronutrients (grams per day) was adjusted based on the total energy intake and participants were divided into quantiles according to their consumption of macronutrients. These quantiles were then used as qualitative variables in the next statistical analyses. Finally, to evaluate the association of macronutrients' intake with the risk of metabolic syndrome and its components, we run multivariate regression after adjusting for the confounding variables such as age, education, gender, physical activity, smoking status, BMI, and family history of Chronic diseases.
Ethical considerations: both YaHS and TAMEZ studies have ethical approval from the Ethics Committee of Shahid Sadoughi University of Medical Sciences. Informed consents were also obtained from all participants.
Results
A cross-sectional study was carried out on 2221 individuals; 529 were afflicted with the MetS and 1692 did not have it. The general characteristics of the study participants are shown in Table 1. The BMI, WC, hip circumference, blood pressure, TG, and FBG were significantly higher in people with MetS. Moreover, 71 percent of the individual with MetS were women over 40 years of age.
A significant difference was observed between individuals with and without metabolic syndrome in terms of physical activity, education, marital status, occupational status, home ownership, and the number of family members. However, no significant difference was observed between the two groups regarding smoking status, ethnicity, house in meters, and the history of chronic diseases.
Table 2 shows the odds ratio of MetS and 95 percent confidence interval for intake of macronutrients in the crude model and after adjusting for the confounding factors in three models.
We adjusted for the confounding variables such as age, education, gender, physical activity, smoking status, BMI, and family history of chronic diseases and found that the odds ratio of MetS was significantly higher in individuals with more intake of carbohydrates (OR: 1.67, CI: 1.01-2.75). However, intake of fat and protein did not have any significant association with the probability of developing MetS (OR: 0.97, CI: 0.59-1.60, OR: 0.90, CI: 0.54-1.49).
Furthermore, individuals with higher intake of carbohydrates had more probability of abdominal obesity (OR: 1.89, CI: 1.06-3.34); whereas, higher consumption of proteins reduced the probability of abdominal obesity (OR: 0.45, CI: 0.25-0.79).
Discussion
Our results showed that the probability of developing MetS in individual with high intake of carbohydrates was 67 percent more than others. Furthermore, high levels of carbohydrate and protein increased and decreased abdominal obesity up to 89 and 55 percent, respectively. To the best of our knowledge, this study was the first research on the association between macronutrients and metabolic syndrome using this number of participants (n = 2221) in Yazd Greater Area. Previous studies in this area presented contradictory results. Similarly, a prospective study on 4152 adult population of China showed that increase in the total intake of carbohydrates, especially starchy foods, could increase the risk of developing MetS significantly (Feng et al., 2015). Moreover, results of cross-sectional studies showed that high intake of carbohydrates and low intake of fats could increase the risk of MetS in women and men (Kwon et al., 2018). In fact, high intake of carbohydrates can inhibit the lipoprotein lipase activity, increase the production of fatty acids in liver cells, increase the levels of triglycerides, and decrease HDL-C levels (Grundy et al., 2002, Nordmann et al., 2006, Song et al., 2012). As a result, it increases the risk of developing MetS.
In addition, the results of a study on the association of high-carbohydrate diet and physical inactivity with abdominal obesity among housewives before their menopause showed a positive correlation between high intake of carbohydrate and WC (Rathnayake et al., 2014). Furthermore, a study on a multi-ethnic population indicated that higher intake of proteins was associated with lower abdominal obesity and WHR (Merchant et al., 2005).
The possible mechanisms for these results may be attributed to the replacement of protein with carbohydrates, which reduces the abdominal obesity in several ways: 1) Postprandial thermogenesis is higher after consuming proteins than carbohydrates (Halton and Hu, 2004); 2) Conjugated linoleic acid, which is abundant in beef and dairy products increases the feeling of satiety in individuals (Kamphuis et al., 2003); 3) Intake of proteins in comparison with carbohydrates improves insulin sensitivity (McAuley et al., 2005) and increases the energy consumption in resting position (Pereira et al., 2004).
However, our results are different from some previous studies. For example, a study on adults population showed that high intake of dietary fat could increase the odds of developing metabolic syndrome. However, no significant relationship was observed between carbohydrate intake and metabolic syndrome (Freire et al., 2005). In a similar study, no correlation was reported between carbohydrate intake and MetS; whereas, intake of whole grains decreased the incidence of MetS (McKeown et al., 2004).
These controversies can be justified by the fact that in the current study, we initially adjusted the amount of macronutrients based on the energy consumption and then conducted the analyses. On the contrary, in other studies energy adjustment was carried out in the final analyses (Kwon et al., 2018, McKeown et al., 2004). Furthermore, individuals' diets and types of consumed carbohydrates are different in various countries. Type and amount of the consumed carbohydrates can play an important role in developing metabolic syndrome. Consequently, these contradictions can be attributed to the difference in intake of refined carbohydrates such as bread without bran, white rice, biscuits, and cakes compared to the whole grains.
The current study has several strong points: the data were collected from the first and largest prospective study in Yazd, which covered a wide range of health-related data, including the urban and rural areas. Furthermore, we used the valid FFQ and evaluated the confounding variables as much as possible. However, some limitations exist in the current study: cross-sectional design that makes us unable to extract the causal inferences. In this regard, we need prospective studies for comprehensive investigations. Despite use of valid FFQ, the measurement error and misclassification of participants may exist.
Ultimately, the data on alcohol consumption were not collected according to the religious sensitivities.
Conclusion
In this cross-sectional study, we concluded that large quantities of carbohydrates increased the risk of getting to MetS and abdominal obesity, while high levels of protein intake reduced the risk. We did not find an association between fat intake and the risk of MetS; so, prospective studies are suggested in this field.
Acknowledgment
We thank the nutrition department in Shahid Sadoughi University of Medical Sciences. We appreciate all who contributed to TAMEZ and YaHS research projects. We are also grateful to the Nutrition and Food Security Research Center Shahid Sadoughi University of Medical Sciences. YaHs and TAMEZ studies were both funded by Shahid Sadoughi University of Medical Sciences
Authors' contributions
Hasanizadeh S and Hosseinzadeh M designed this study. Hasanizadeh S, Hosseinzadeh M, and Salehi Abarghouei A cooperated in statistical analysis of this study. Hasanizadeh S wrote the initial draft of this manuscript. Other authors edited the draft and all the authors approved the final version for submit.
Conflict of interests
The authors declare no conflict of interest regarding this study.
References
Alberti K, et al. 2009. Harmonizing the metabolic syndrome: a joint interim statement of the international diabetes federation task force on epidemiology and prevention; national heart, lung, and blood institute; American heart association; world heart federation; international atherosclerosis society; and international association for the study of obesity. Circulation. 120 (16): 1640-1645.
Azadbakht L, Mirmiran P, Esmaillzadeh A, Azizi T & Azizi F 2005. Beneficial effects of a Dietary Approaches to Stop Hypertension eating plan on features of the metabolic syndrome. Diabetes care. 28 (12): 2823-2831.
Carnethon MR, et al. 2004. Risk factors for the metabolic syndrome: the Coronary Artery Risk Development in Young Adults (CARDIA) study, 1985–2001. Diabetes care. 27 (11): 2707-2715.
Casas-Agustench P, et al. 2011. Effects of one serving of mixed nuts on serum lipids, insulin resistance and inflammatory markers in patients with the metabolic syndrome. Nutrition, metabolism and cardiovascular diseases. 21 (2): 126-135.
Dalvand S, et al. 2017. Prevalence of metabolic syndrome among iranian population: A systematic review and meta-analysis. Iranian journal of public health. 46 (4): 456.
Delavari A, Forouzanfar MH, Alikhani S, Sharifian A & Kelishadi R 2009. The First nationwide study of the prevalence of the metabolic syndrome and optimal cut-off points of waist circumference in the middle east: the national survey of risk factors for non-communicable diseases of Iran. Diabetes care. 32: 6.
Eilat-Adar S, et al. 2008. Sex may modify the effects of macronutrient intake on metabolic syndrome and insulin resistance in American Indians: the strong heart study. Journal of the American dietetic association. 108 (5): 794-802.
Esmaillzadeh A, Mirmiran P & Azizi F 2005. Whole-grain consumption and the metabolic syndrome: a favorable association in Tehranian adults. European journal of clinical nutrition. 59 (3): 353.
Esposito K & Giugliano D 2010. Mediterranean diet and the metabolic syndrome: the end of the beginning. Metabolic syndrome and related disorders. 8 (3): 197-200.
Feng R, et al. 2015. High carbohydrate intake from starchy foods is positively associated with metabolic disorders: a Cohort Study from a Chinese population. Scientific reports. 5 (1): 1-8.
Freire RD, Cardoso MA, Gimeno SG & Ferreira SR 2005. Dietary fat is associated with metabolic syndrome in Japanese Brazilians. Diabetes care. 28 (7): 1779-1785.
Ghaffarpour M, Houshiar-Rad A & Kianfar H 1999. The manual for household measures, cooking yields factors and edible portion of foods. p. 213: Tehran: Nashre Olume Keshavarzy.
Grundy SM, Abate N & Chandalia M 2002. Diet composition and the metabolic syndrome: what is the optimal fat intake? American journal of medicine. 113 (9): 25-29.
Halton TL & Hu FB 2004. The effects of high protein diets on thermogenesis, satiety and weight loss: a critical review. Journal of the American college of nutrition. 23 (5): 373-385.
Johnson RJ, et al. 2007. Potential role of sugar (fructose) in the epidemic of hypertension, obesity and the metabolic syndrome, diabetes, kidney disease, and cardiovascular disease–. American journal of clinical nutrition. 86 (4): 899-906.
Kamphuis MM, Lejeune MP, Saris WH & Westerterp-Plantenga MS 2003. Effect of conjugated linoleic acid supplementation after weight loss on appetite and food intake in overweight subjects. European journal of clinical nutrition. 57 (10): 1268.
Kaur J 2014. Assessment and screening of the risk factors in metabolic syndrome. Medical sciences. 2 (3): 140-152.
Kolovou GD, Anagnostopoulou KK, Salpea KD & Mikhailidis DP 2007. The prevalence of metabolic syndrome in various populations. American journal of the medical sciences. 333 (6): 362-371.
Kwon Y-J, Lee H-S & Lee J-W 2018. Association of carbohydrate and fat intake with metabolic syndrome. Clinical nutrition. 37 (2): 746-751.
Lakka H-M, et al. 2002. The metabolic syndrome and total and cardiovascular disease mortality in middle-aged men. Journal of the American medical association. 288 (21): 2709-2716.
Linardakis M, Bertsias G, Sarri K, Papadaki A & Kafatos A 2008. Metabolic syndrome in children and adolescents in Crete, Greece, and association with diet quality and physical fitness. Journal of public health. 16 (6): 421-428.
McAuley K, et al. 2005. Comparison of high-fat and high-protein diets with a high-carbohydrate diet in insulin-resistant obese women. Diabetologia. 48 (1): 8-16.
McKeown NM, et al. 2004. Carbohydrate nutrition, insulin resistance, and the prevalence of the metabolic syndrome in the Framingham Offspring Cohort. Diabetes care. 27 (2): 538-546.
Merchant AT, et al. 2005. Protein intake is inversely associated with abdominal obesity in a multi-ethnic population. Journal of nutrition. 135 (5): 1196-1201.
Mirzaei M, Salehi-Abargouei A, Mirzaei M & Mohsenpour MA 2017. Cohort Profile: The Yazd Health Study (YaHS): a population-based study of adults aged 20–70 years (study design and baseline population data). International journal of epidemiology. 47 (3): 697-698h.
Mittendorfer B & Sidossis LS 2001. Mechanism for the increase in plasma triacylglycerol concentrations after consumption of short-term, high-carbohydrate diets–. American journal of clinical nutrition. 73 (5): 892-899.
Nordmann AJ, et al. 2006. Effects of low-carbohydrate vs low-fat diets on weight loss and cardiovascular risk factors: a meta-analysis of randomized controlled trials. Archives of internal medicine. 166 (3): 285-293.
Pereira MA, Swain J, Goldfine AB, Rifai N & Ludwig DS 2004. Effects of a low–glycemic load diet on resting energy expenditure and heart disease risk factors during weight loss. Journal of the American medical association. 292 (20): 2482-2490.
Povel CM, et al. 2012. Single nucleotide polymorphisms (SNPs) involved in insulin resistance, weight regulation, lipid metabolism and inflammation in relation to metabolic syndrome: an epidemiological study. Cardiovascular diabetology. 11 (1): 133.
Rathnayake KM, Roopasingam T & Dibley MJ 2014. High carbohydrate diet and physical inactivity associated with central obesity among premenopausal housewives in Sri Lanka. BMC research notes. 7 (1): 564.
Skilton MR, Laville M, Cust AE, Moulin P & Bonnet F 2008. The association between dietary macronutrient intake and the prevalence of the metabolic syndrome. British journal of nutrition. 100 (2): 400-407.
Song Y, et al. 2012. Effects of a low-fat and high-carbohydrate diet on the physiological and biochemical indices in healthy youth with different body mass index. Journal of Sichuan University. medical science edition. 43 (1): 9-14
Our results showed that the probability of developing MetS in individual with high intake of carbohydrates was 67 percent more than others. Furthermore, high levels of carbohydrate and protein increased and decreased abdominal obesity up to 89 and 55 percent, respectively. To the best of our knowledge, this study was the first research on the association between macronutrients and metabolic syndrome using this number of participants (n = 2221) in Yazd Greater Area. Previous studies in this area presented contradictory results. Similarly, a prospective study on 4152 adult population of China showed that increase in the total intake of carbohydrates, especially starchy foods, could increase the risk of developing MetS significantly (Feng et al., 2015). Moreover, results of cross-sectional studies showed that high intake of carbohydrates and low intake of fats could increase the risk of MetS in women and men (Kwon et al., 2018). In fact, high intake of carbohydrates can inhibit the lipoprotein lipase activity, increase the production of fatty acids in liver cells, increase the levels of triglycerides, and decrease HDL-C levels (Grundy et al., 2002, Nordmann et al., 2006, Song et al., 2012). As a result, it increases the risk of developing MetS.
In addition, the results of a study on the association of high-carbohydrate diet and physical inactivity with abdominal obesity among housewives before their menopause showed a positive correlation between high intake of carbohydrate and WC (Rathnayake et al., 2014). Furthermore, a study on a multi-ethnic population indicated that higher intake of proteins was associated with lower abdominal obesity and WHR (Merchant et al., 2005).
The possible mechanisms for these results may be attributed to the replacement of protein with carbohydrates, which reduces the abdominal obesity in several ways: 1) Postprandial thermogenesis is higher after consuming proteins than carbohydrates (Halton and Hu, 2004); 2) Conjugated linoleic acid, which is abundant in beef and dairy products increases the feeling of satiety in individuals (Kamphuis et al., 2003); 3) Intake of proteins in comparison with carbohydrates improves insulin sensitivity (McAuley et al., 2005) and increases the energy consumption in resting position (Pereira et al., 2004).
However, our results are different from some previous studies. For example, a study on adults population showed that high intake of dietary fat could increase the odds of developing metabolic syndrome. However, no significant relationship was observed between carbohydrate intake and metabolic syndrome (Freire et al., 2005). In a similar study, no correlation was reported between carbohydrate intake and MetS; whereas, intake of whole grains decreased the incidence of MetS (McKeown et al., 2004).
These controversies can be justified by the fact that in the current study, we initially adjusted the amount of macronutrients based on the energy consumption and then conducted the analyses. On the contrary, in other studies energy adjustment was carried out in the final analyses (Kwon et al., 2018, McKeown et al., 2004). Furthermore, individuals' diets and types of consumed carbohydrates are different in various countries. Type and amount of the consumed carbohydrates can play an important role in developing metabolic syndrome. Consequently, these contradictions can be attributed to the difference in intake of refined carbohydrates such as bread without bran, white rice, biscuits, and cakes compared to the whole grains.
The current study has several strong points: the data were collected from the first and largest prospective study in Yazd, which covered a wide range of health-related data, including the urban and rural areas. Furthermore, we used the valid FFQ and evaluated the confounding variables as much as possible. However, some limitations exist in the current study: cross-sectional design that makes us unable to extract the causal inferences. In this regard, we need prospective studies for comprehensive investigations. Despite use of valid FFQ, the measurement error and misclassification of participants may exist.
Ultimately, the data on alcohol consumption were not collected according to the religious sensitivities.
Conclusion
In this cross-sectional study, we concluded that large quantities of carbohydrates increased the risk of getting to MetS and abdominal obesity, while high levels of protein intake reduced the risk. We did not find an association between fat intake and the risk of MetS; so, prospective studies are suggested in this field.
Acknowledgment
We thank the nutrition department in Shahid Sadoughi University of Medical Sciences. We appreciate all who contributed to TAMEZ and YaHS research projects. We are also grateful to the Nutrition and Food Security Research Center Shahid Sadoughi University of Medical Sciences. YaHs and TAMEZ studies were both funded by Shahid Sadoughi University of Medical Sciences
Authors' contributions
Hasanizadeh S and Hosseinzadeh M designed this study. Hasanizadeh S, Hosseinzadeh M, and Salehi Abarghouei A cooperated in statistical analysis of this study. Hasanizadeh S wrote the initial draft of this manuscript. Other authors edited the draft and all the authors approved the final version for submit.
Conflict of interests
The authors declare no conflict of interest regarding this study.
References
Alberti K, et al. 2009. Harmonizing the metabolic syndrome: a joint interim statement of the international diabetes federation task force on epidemiology and prevention; national heart, lung, and blood institute; American heart association; world heart federation; international atherosclerosis society; and international association for the study of obesity. Circulation. 120 (16): 1640-1645.
Azadbakht L, Mirmiran P, Esmaillzadeh A, Azizi T & Azizi F 2005. Beneficial effects of a Dietary Approaches to Stop Hypertension eating plan on features of the metabolic syndrome. Diabetes care. 28 (12): 2823-2831.
Carnethon MR, et al. 2004. Risk factors for the metabolic syndrome: the Coronary Artery Risk Development in Young Adults (CARDIA) study, 1985–2001. Diabetes care. 27 (11): 2707-2715.
Casas-Agustench P, et al. 2011. Effects of one serving of mixed nuts on serum lipids, insulin resistance and inflammatory markers in patients with the metabolic syndrome. Nutrition, metabolism and cardiovascular diseases. 21 (2): 126-135.
Dalvand S, et al. 2017. Prevalence of metabolic syndrome among iranian population: A systematic review and meta-analysis. Iranian journal of public health. 46 (4): 456.
Delavari A, Forouzanfar MH, Alikhani S, Sharifian A & Kelishadi R 2009. The First nationwide study of the prevalence of the metabolic syndrome and optimal cut-off points of waist circumference in the middle east: the national survey of risk factors for non-communicable diseases of Iran. Diabetes care. 32: 6.
Eilat-Adar S, et al. 2008. Sex may modify the effects of macronutrient intake on metabolic syndrome and insulin resistance in American Indians: the strong heart study. Journal of the American dietetic association. 108 (5): 794-802.
Esmaillzadeh A, Mirmiran P & Azizi F 2005. Whole-grain consumption and the metabolic syndrome: a favorable association in Tehranian adults. European journal of clinical nutrition. 59 (3): 353.
Esposito K & Giugliano D 2010. Mediterranean diet and the metabolic syndrome: the end of the beginning. Metabolic syndrome and related disorders. 8 (3): 197-200.
Feng R, et al. 2015. High carbohydrate intake from starchy foods is positively associated with metabolic disorders: a Cohort Study from a Chinese population. Scientific reports. 5 (1): 1-8.
Freire RD, Cardoso MA, Gimeno SG & Ferreira SR 2005. Dietary fat is associated with metabolic syndrome in Japanese Brazilians. Diabetes care. 28 (7): 1779-1785.
Ghaffarpour M, Houshiar-Rad A & Kianfar H 1999. The manual for household measures, cooking yields factors and edible portion of foods. p. 213: Tehran: Nashre Olume Keshavarzy.
Grundy SM, Abate N & Chandalia M 2002. Diet composition and the metabolic syndrome: what is the optimal fat intake? American journal of medicine. 113 (9): 25-29.
Halton TL & Hu FB 2004. The effects of high protein diets on thermogenesis, satiety and weight loss: a critical review. Journal of the American college of nutrition. 23 (5): 373-385.
Johnson RJ, et al. 2007. Potential role of sugar (fructose) in the epidemic of hypertension, obesity and the metabolic syndrome, diabetes, kidney disease, and cardiovascular disease–. American journal of clinical nutrition. 86 (4): 899-906.
Kamphuis MM, Lejeune MP, Saris WH & Westerterp-Plantenga MS 2003. Effect of conjugated linoleic acid supplementation after weight loss on appetite and food intake in overweight subjects. European journal of clinical nutrition. 57 (10): 1268.
Kaur J 2014. Assessment and screening of the risk factors in metabolic syndrome. Medical sciences. 2 (3): 140-152.
Kolovou GD, Anagnostopoulou KK, Salpea KD & Mikhailidis DP 2007. The prevalence of metabolic syndrome in various populations. American journal of the medical sciences. 333 (6): 362-371.
Kwon Y-J, Lee H-S & Lee J-W 2018. Association of carbohydrate and fat intake with metabolic syndrome. Clinical nutrition. 37 (2): 746-751.
Lakka H-M, et al. 2002. The metabolic syndrome and total and cardiovascular disease mortality in middle-aged men. Journal of the American medical association. 288 (21): 2709-2716.
Linardakis M, Bertsias G, Sarri K, Papadaki A & Kafatos A 2008. Metabolic syndrome in children and adolescents in Crete, Greece, and association with diet quality and physical fitness. Journal of public health. 16 (6): 421-428.
McAuley K, et al. 2005. Comparison of high-fat and high-protein diets with a high-carbohydrate diet in insulin-resistant obese women. Diabetologia. 48 (1): 8-16.
McKeown NM, et al. 2004. Carbohydrate nutrition, insulin resistance, and the prevalence of the metabolic syndrome in the Framingham Offspring Cohort. Diabetes care. 27 (2): 538-546.
Merchant AT, et al. 2005. Protein intake is inversely associated with abdominal obesity in a multi-ethnic population. Journal of nutrition. 135 (5): 1196-1201.
Mirzaei M, Salehi-Abargouei A, Mirzaei M & Mohsenpour MA 2017. Cohort Profile: The Yazd Health Study (YaHS): a population-based study of adults aged 20–70 years (study design and baseline population data). International journal of epidemiology. 47 (3): 697-698h.
Mittendorfer B & Sidossis LS 2001. Mechanism for the increase in plasma triacylglycerol concentrations after consumption of short-term, high-carbohydrate diets–. American journal of clinical nutrition. 73 (5): 892-899.
Nordmann AJ, et al. 2006. Effects of low-carbohydrate vs low-fat diets on weight loss and cardiovascular risk factors: a meta-analysis of randomized controlled trials. Archives of internal medicine. 166 (3): 285-293.
Pereira MA, Swain J, Goldfine AB, Rifai N & Ludwig DS 2004. Effects of a low–glycemic load diet on resting energy expenditure and heart disease risk factors during weight loss. Journal of the American medical association. 292 (20): 2482-2490.
Povel CM, et al. 2012. Single nucleotide polymorphisms (SNPs) involved in insulin resistance, weight regulation, lipid metabolism and inflammation in relation to metabolic syndrome: an epidemiological study. Cardiovascular diabetology. 11 (1): 133.
Rathnayake KM, Roopasingam T & Dibley MJ 2014. High carbohydrate diet and physical inactivity associated with central obesity among premenopausal housewives in Sri Lanka. BMC research notes. 7 (1): 564.
Skilton MR, Laville M, Cust AE, Moulin P & Bonnet F 2008. The association between dietary macronutrient intake and the prevalence of the metabolic syndrome. British journal of nutrition. 100 (2): 400-407.
Song Y, et al. 2012. Effects of a low-fat and high-carbohydrate diet on the physiological and biochemical indices in healthy youth with different body mass index. Journal of Sichuan University. medical science edition. 43 (1): 9-14
Type of article: orginal article |
Subject:
public specific
Received: 2019/08/25 | Published: 2020/02/1 | ePublished: 2020/02/1
Received: 2019/08/25 | Published: 2020/02/1 | ePublished: 2020/02/1
References
1. Alberti K, et al. 2009. Harmonizing the metabolic syndrome: a joint interim statement of the international diabetes federation task force on epidemiology and prevention; national heart, lung, and blood institute; American heart association; world heart federation; international atherosclerosis society; and international association for the study of obesity. Circulation. 120 (16): 1640-1645.
2. Azadbakht L, Mirmiran P, Esmaillzadeh A, Azizi T & Azizi F 2005. Beneficial effects of a Dietary Approaches to Stop Hypertension eating plan on features of the metabolic syndrome. Diabetes care. 28 (12): 2823-2831.
3. Carnethon MR, et al. 2004. Risk factors for the metabolic syndrome: the Coronary Artery Risk Development in Young Adults (CARDIA) study, 1985–2001. Diabetes care. 27 (11): 2707-2715.
4. Casas-Agustench P, et al. 2011. Effects of one serving of mixed nuts on serum lipids, insulin resistance and inflammatory markers in patients with the metabolic syndrome. Nutrition, metabolism and cardiovascular diseases. 21 (2): 126-135.
5. Dalvand S, et al. 2017. Prevalence of metabolic syndrome among iranian population: A systematic review and meta-analysis. Iranian journal of public health. 46 (4): 456.
6. Delavari A, Forouzanfar MH, Alikhani S, Sharifian A & Kelishadi R 2009. The First nationwide study of the prevalence of the metabolic syndrome and optimal cut-off points of waist circumference in the middle east: the national survey of risk factors for non-communicable diseases of Iran. Diabetes care. 32: 6.
7. Eilat-Adar S, et al. 2008. Sex may modify the effects of macronutrient intake on metabolic syndrome and insulin resistance in American Indians: the strong heart study. Journal of the American dietetic association. 108 (5): 794-802.
8. Esmaillzadeh A, Mirmiran P & Azizi F 2005. Whole-grain consumption and the metabolic syndrome: a favorable association in Tehranian adults. European journal of clinical nutrition. 59 (3): 353.
9. Esposito K & Giugliano D 2010. Mediterranean diet and the metabolic syndrome: the end of the beginning. Metabolic syndrome and related disorders. 8 (3): 197-200.
10. Feng R, et al. 2015. High carbohydrate intake from starchy foods is positively associated with metabolic disorders: a Cohort Study from a Chinese population. Scientific reports. 5 (1): 1-8.
11. Freire RD, Cardoso MA, Gimeno SG & Ferreira SR 2005. Dietary fat is associated with metabolic syndrome in Japanese Brazilians. Diabetes care. 28 (7): 1779-1785.
12. Ghaffarpour M, Houshiar-Rad A & Kianfar H 1999. The manual for household measures, cooking yields factors and edible portion of foods. p. 213: Tehran: Nashre Olume Keshavarzy.
13. Grundy SM, Abate N & Chandalia M 2002. Diet composition and the metabolic syndrome: what is the optimal fat intake? American journal of medicine. 113 (9): 25-29.
14. Halton TL & Hu FB 2004. The effects of high protein diets on thermogenesis, satiety and weight loss: a critical review. Journal of the American college of nutrition. 23 (5): 373-385.
15. Johnson RJ, et al. 2007. Potential role of sugar (fructose) in the epidemic of hypertension, obesity and the metabolic syndrome, diabetes, kidney disease, and cardiovascular disease–. American journal of clinical nutrition. 86 (4): 899-906.
16. Kamphuis MM, Lejeune MP, Saris WH & Westerterp-Plantenga MS 2003. Effect of conjugated linoleic acid supplementation after weight loss on appetite and food intake in overweight subjects. European journal of clinical nutrition. 57 (10): 1268.
17. Kaur J 2014. Assessment and screening of the risk factors in metabolic syndrome. Medical sciences. 2 (3): 140-152.
18. Kolovou GD, Anagnostopoulou KK, Salpea KD & Mikhailidis DP 2007. The prevalence of metabolic syndrome in various populations. American journal of the medical sciences. 333 (6): 362-371.
19. Kwon Y-J, Lee H-S & Lee J-W 2018. Association of carbohydrate and fat intake with metabolic syndrome. Clinical nutrition. 37 (2): 746-751.
20. Lakka H-M, et al. 2002. The metabolic syndrome and total and cardiovascular disease mortality in middle-aged men. Journal of the American medical association. 288 (21): 2709-2716.
21. Linardakis M, Bertsias G, Sarri K, Papadaki A & Kafatos A 2008. Metabolic syndrome in children and adolescents in Crete, Greece, and association with diet quality and physical fitness. Journal of public health. 16 (6): 421-428.
22. McAuley K, et al. 2005. Comparison of high-fat and high-protein diets with a high-carbohydrate diet in insulin-resistant obese women. Diabetologia. 48 (1): 8-16.
23. McKeown NM, et al. 2004. Carbohydrate nutrition, insulin resistance, and the prevalence of the metabolic syndrome in the Framingham Offspring Cohort. Diabetes care. 27 (2): 538-546.
24. Merchant AT, et al. 2005. Protein intake is inversely associated with abdominal obesity in a multi-ethnic population. Journal of nutrition. 135 (5): 1196-1201.
25. Mirzaei M, Salehi-Abargouei A, Mirzaei M & Mohsenpour MA 2017. Cohort Profile: The Yazd Health Study (YaHS): a population-based study of adults aged 20–70 years (study design and baseline population data). International journal of epidemiology. 47 (3): 697-698h.
26. Mittendorfer B & Sidossis LS 2001. Mechanism for the increase in plasma triacylglycerol concentrations after consumption of short-term, high-carbohydrate diets–. American journal of clinical nutrition. 73 (5): 892-899.
27. Nordmann AJ, et al. 2006. Effects of low-carbohydrate vs low-fat diets on weight loss and cardiovascular risk factors: a meta-analysis of randomized controlled trials. Archives of internal medicine. 166 (3): 285-293.
28. Pereira MA, Swain J, Goldfine AB, Rifai N & Ludwig DS 2004. Effects of a low–glycemic load diet on resting energy expenditure and heart disease risk factors during weight loss. Journal of the American medical association. 292 (20): 2482-2490.
29. Povel CM, et al. 2012. Single nucleotide polymorphisms (SNPs) involved in insulin resistance, weight regulation, lipid metabolism and inflammation in relation to metabolic syndrome: an epidemiological study. Cardiovascular diabetology. 11 (1): 133.
30. Rathnayake KM, Roopasingam T & Dibley MJ 2014. High carbohydrate diet and physical inactivity associated with central obesity among premenopausal housewives in Sri Lanka. BMC research notes. 7 (1): 564.
31. Skilton MR, Laville M, Cust AE, Moulin P & Bonnet F 2008. The association between dietary macronutrient intake and the prevalence of the metabolic syndrome. British journal of nutrition. 100 (2): 400-407.
32. Song Y, et al. 2012. Effects of a low-fat and high-carbohydrate diet on the physiological and biochemical indices in healthy youth with different body mass index. Journal of Sichuan University. medical science edition. 43 (1): 9-14
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
